INTRODUCTION
In the era of highly active antiretroviral therapy (HAART), human immunodeficiency virus (HIV) infection is considered a chronic rather than a fatal disease [1]. HAART effectively prevents the development of acquired immune deficiency syndrome (AIDS) and opportunistic infections, thus providing HIV/AIDS patients an extended life expectancy with improved quality of life [2]. Despite prolonged life expectancy, the suicide rate in HIV/AIDS patients is still higher than that in the general population [3]. Especially in South Korea, misunderstanding and prejudice against HIV/AIDS patients leads to them suffering social isolation and stigmatization, thus causing depression and suicidal ideation [4]. Patients with stable HIV infection are mainly managed in outpatient clinics with regular follow-up, and are prescribed long-term medications for more than a month. If the patients have any suicidal ideation, there could be a potential risk of poisoning through prescribed medications, especially using antiviral agents.
Atazanavir (Reyataz; Bristol-Myers Squibb, Princeton, NJ, USA), a protease inhibitor, is approved in many countries for use as a component of HAART regimens in the treatment of patients with HIV-1 infection [5]. The most common adverse events of atazanavir are nausea, jaundice, and diarrhea. However, among less common adverse events, prolongation of the PR interval and corrected QT (QTc) have been reported in some patients [6]. There have been 3 case reports of atazanavir-related torsades de pointes and 1 case report of ventricular tachycardia with QTc prolongation [7-9]. The 4 patients involved had severe comorbidities, such as heart failure, liver cirrhosis, and intravenous drug usage. Here, we present the case of a 40-year-old HIV-1-infected man who presented with monomorphic ventricular tachycardia. He had no comorbidities, except for HIV-1 infection, and took 150 atazanavir capsules (200 mg atazanavir per capsule) with a suicidal intent.
CASE REPORT
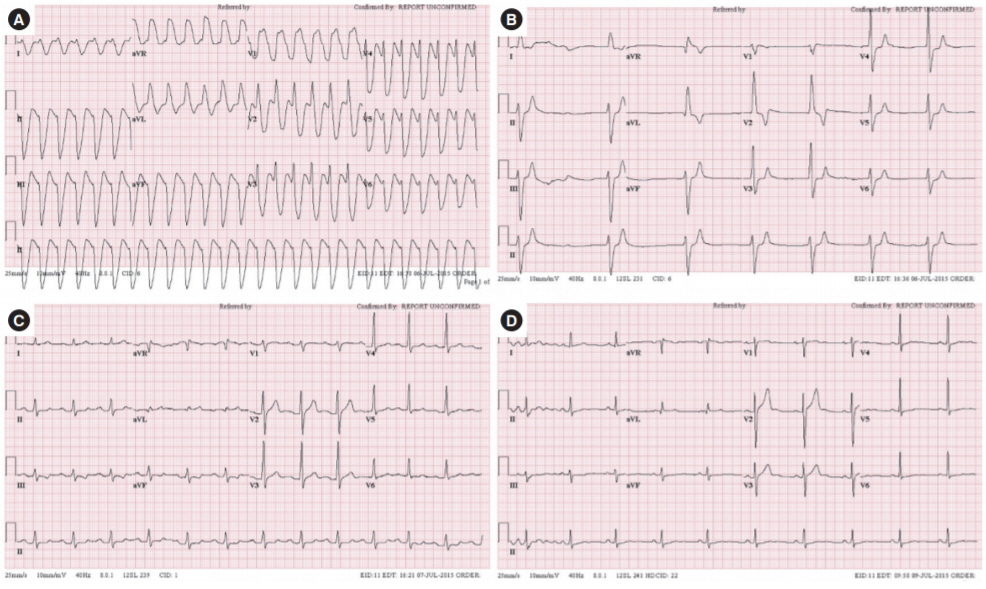
A 40-year-old HIV-1-infected man presented to the emergency department with syncope and palpitations. He admitted to taking 150 atazanavir capsules (200 mg atazanavir per capsule) with the purpose of attempting suicide 3 days previously. His initial blood pressure was 119/75 mmHg, and his heart rate was 152 beats/min. The patient’s initial 12-lead electrocardiogram (ECG) revealed ventricular tachycardia with prolonged QTc of 441 ms (Fig. 1A). Thirty minutes after a 10% magnesium sulfate infusion (2 g), his ECG rhythm converted to junctional bradycardia (Fig. 1B) with a heart rate of 41 beats/min, and the palpitations had improved. He was admitted to the emergency intensive care unit for close observation.
In his initial electrolyte panel, sodium, potassium, chloride, and total CO2 levels were 132, 4.3, 100, and 16 mmol/L, respectively. His initial serum magnesium level was 1.7 mEq/L. Initial admission panel results were unremarkable, except for elevated total bilirubin (10.0 mg/dL) and creatinine (1.94 mg/dL). After 6 hours of observation and administration of normal saline (80 mL/hr), his ECG rhythm converted to sinus rhythm with 1st degree atrioventricular block (Fig. 1C). During his hospital stay, his QTc time, PR interval and total bilirubin level decreased (Table 1). On day 2 of his hospital stay, a 2-D echocardiography undertaken by a cardiologist revealed that his ejection fraction was 65%, but it did not reveal any other abnormalities. By day 3, his ECG had completely normalized (Fig. 1D) and the elevated total bilirubin level had decreased to 0.7 mg/dL. He was discharged from the hospital general ward on day 3, following a psychiatric consultation and an antiviral regimen change.
DISCUSSION
Prolongation of the QT interval for more than 500 ms increases the risk of torsades de pointes [10]. Protease inhibitors, including atazanavir, and many other drugs cause QT prolongation through a blockade of the human ether-a-go-go–related gene potassium ion channel, which regulates a major repolarizing potassium current [11]. Among the previous 4 cases with atazanavir toxicity in which torsades de pointes or ventricular tachycardia developed, one patient had congestive heart failure and was undergoing hemodialysis [7]. Two patients used methadone, which also induces QT interval prolongation, and electrical defibrillation was delivered for the termination of torsades de pointes [8]. In the last of the four cases, the patient had liver cirrhosis and doubled his usual dosage of oxycodone, which can induce a drug interaction with atazanavir, and electrical defibrillation was delivered for the termination of torsades de pointes [9].
To our knowledge, this is the first case of atazanavir intoxication in an HIV patient with suicidal intent. Unlike the previous cases, in which electrical defibrillation was delivered for the termination of ventricular arrhythmia, we used MgSO4 as an initial antiarrhythmic drug, and soon after the MgSO4 infusion, the patient’s ventricular tachycardia was terminated. In cases of torsades de pointes induced by drug intoxication, magnesium should be considered as the first antiarrhythmic drug [12]. Magnesium can also be used in cases of sustained monomorphic ventricular tachycardia that are unresponsive to a first-line drug such as amiodarone [13]. In the present case, we used magnesium as an initial antiarrhythmic drug because, in the brief period of initial assessment, we searched previous cases reports in which QTc prolongation was identified as a possible severe side effect of atazanavir use. Considering the patient’s initial prolonged QTc interval, there was a risk of developing torsades de pointes or more severe ventricular arrhythmia. After the infusion of MgSO4, the patient’s monomorphic ventricular tachycardia was converted to an atrioventricular nodal rhythm, and the patient’s palpitation symptoms disappeared.
Uglietti et al. [14] reported that the level of hyperbilirubinemia is related to the toxicity level of atazanavir in the early medication initiation period. We used the total bilirubin level as an indicator of serum atazanavir levels. As the patient’s total bilirubin level decreased to a normal range, the PR interval and QTc time were also normalized.
In summary, monomorphic ventricular tachycardia was induced by atazanavir intoxication and was terminated soon after MgSO4 infusion. Through normal saline hydration and the withdrawal of atazanavir, the patient’s QTc prolongation and hyperbilirubinemia were improved at the same time. In South Korea, where the number of HIV/AIDS patients is increasing and the suicide rate is high, physicians should be aware that poisoning using HAART medication can occur in susceptible patients, and QTc prolongation or ventricular arrhythmia can be induced by protease inhibitors.