INTRODUCTION
Major hemorrhage remains a leading cause of early death after severe trauma [1]. In addition to immediate identification of bleeding sources and the appropriate hemostatic intervention, early transfusion can prevent the development of acute traumatic coagulopathy and improve survival [2-5]. Delayed recognition and control of active hemorrhage is among the major causes of preventable death from trauma [6].
Several scoring systems have been developed to predict the need for massive transfusion (MT) in severely injured trauma patients. These systems incorporate several clinical parameters including age, vital signs, laboratory data, and ultrasound or pelvic X-ray findings [7-12]. As whole-body computed tomography (CT) scanning in severely injured trauma patients has been shown to yield beneficial outcomes and is commonly performed in current trauma practice, specific CT findings may be helpful in determining the need for MT. The inferior vena cava (IVC) diameter on the initial CT image has been reported to be a potential predictor of mortality or the necessity for MT [2,13-15].
Although decreased pancreatic perfusion in the early phase and delayed pancreatic enhancement in the late phase have been shown to be associated with hypovolemic shock, the significance of enhanced computed tomography attenuation values (CTAVs) of major vessels has not been elucidated [16]. Therefore, this study aimed to investigate the usefulness of enhanced CTAV of major vessels as a predictor of MT in patients with major blunt trauma. We hypothesized that the enhanced CTAV of major vessels such as the aorta would be higher in patients requiring MT due to lower cardiac output.
METHODS
Study design and participants
This single-center retrospective study reviewed the trauma registry and medical records of consecutive trauma patients admitted to our tertiary hospital between April 2014 and March 2018. Patients younger than 16 years old and those with cardiac arrest on arrival, penetrating mechanism of injury, Injury Severity Score of less than 9, and those who had not undergone contrast-enhanced CT scans of the torso were excluded. Patients who had been administered contrast material intravenously through the lower extremity were also excluded. This study was approved by the ethics committee of Okayama University Hospital (1807-015). The requirement for written informed consent was waived due to the retrospective nature of the study.
Patient management
In our hospital, whole-body CT scanning, including native CT examination of the head, neck, and torso (i.e., chest, abdomen, and pelvis), is performed during the initial evaluation of blunt torso trauma patients, regardless of hemodynamic status. This is followed by enhanced CT scanning of the torso in hemodynamically unstable patients and those with high-energy trauma. After bleeding sources are identified and the hemorrhage is successfully controlled via surgical and/or catheter intervention, the necessity for MT is determined based on clinical judgment. Patients who are identified to need MT received transfusions of red blood cells (RBCs), fresh frozen plasma, and platelet concentrates at a 1:1:1 ratio as soon as possible.
CT examination protocol
CT imaging was performed using an Aquilion 64-row multi-slice CT (Toshiba Medical Systems, Okayama, Japan) with the following imaging parameters: tube voltage, 120 kV; tube current, 300 mA; slice thickness, 5 mm; and gantry rotation time, 0.75 seconds. After obtaining native scans of the head, neck, and torso (i.e., chest, abdomen, pelvis), contrast-enhanced CT of the torso combining the arterial and portal venous phases was obtained. A total of either 100, 125, 135, or 150 mL contrast material and iodine concentrations of either 300, 350, or 370 mg iodine/mL (ideally, 500 to 600 mg iodine/kg) were administered within 30 seconds through peripheral venous access in the upper extremity based on the estimated body weight. Patients underwent scans of 5-mm-thick sections of the torso during the arterial and portal venous phases, which were conducted 30 and 80 seconds after the start of the injection of contrast material, respectively.
CT measured contrast attenuation values of the major vessels
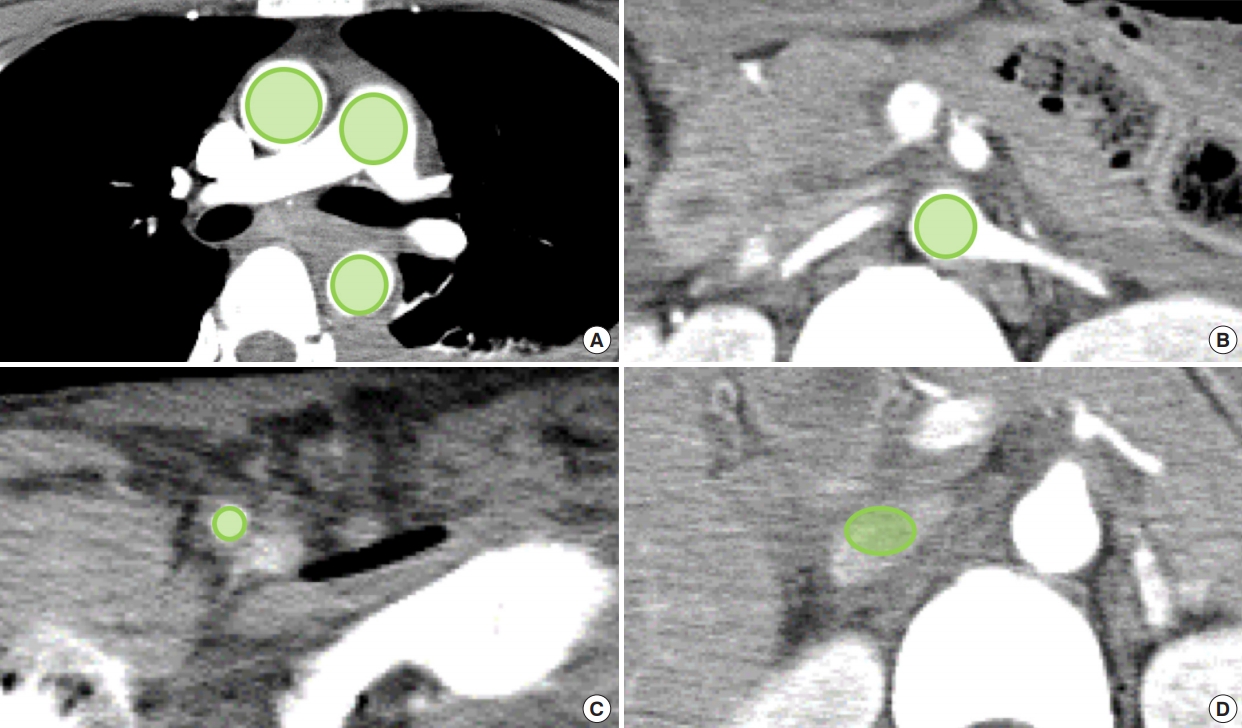
The mean Hounsfield unit (HU) density was quantified by using an elliptical region-of-interest tool of a commercially available viewer software package (Synapse ver. 4.1, Fujifilm Medical, Tokyo, Japan) [16-18]. Given the measurability and application for clinical practice, we selected six major vessel points in both the arterial and portal venous phases to determine predictability and reliability, namely, 1) the main pulmonary artery at the level of its bifurcation; 2, 3) the ascending aorta and descending aorta at the level of main pulmonary artery bifurcation; 4) the abdominal aorta at the left renal artery branching level; 5) the common femoral artery on the right; and 6) the IVC 25 mm (5 slices) above the right renal vein (Fig. 1). Cross-sectional largest possible areas of each vessel were measured, avoiding the edges of the vessels to prevent partial volume effect caused by calcified plaques [16-18]. The left common femoral artery was evaluated to confirm correct placement of the catheter. The CTAV of IVC or the abdominal aorta was traced, avoiding the area where the catheter had been placed.
CTAVs were measured twice by two emergency physicians (a senior resident and an attending physician) who were unaware of the patientŌĆÖs outcomes. The means of the two measurements were then analyzed.
Data collection
Demographic information and clinical data, including mechanism of injury, vital signs, base excess, lactate level, coagulation markers on emergency department arrival, Injury Severity Score, associated injuries, blood products received, treatment, patient outcomes, and enhanced CTAV of major vessels, were collected. As the degree of contrast enhancement is affected by body weight and total iodine used, an additional analysis was conducted using CTAV adjusted by iodine dose per body weight [19]. MT was defined as a transfusion of 8 or more units of RBCs within the first 6 hours after the patientŌĆÖs arrival at the hospital because the traditional MT concept (10 units or more of RBCs within 24 hours) has been shown to be imprecise due to survivorship bias [20-22].
Statistical analysis
Continuous variables were described as median and interquartile range and categorical variables as frequencies or percentages. Univariate analyses were performed using Fisher exact probability test and Mann-Whitney U-test as appropriate. Intraclass correlation analysis was used to determine the interobserver agreement of the enhanced CTAV measurements. Spearman correlation coefficients were computed to compare the relationship between enhanced CTAV and physiological parameters. The capability of enhanced CTAV to predict the necessity for MT was estimated based on the area under the receiver operating characteristic curve (AUROC). The optimal cut-off value was explored using the Youden index. A two-tailed P-value of <0.05 was considered statistically significant. All analyses were conducted using IBM SPSS Statistics ver. 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Study population and characteristics
In total, 679 trauma patients were admitted to our tertiary hospital during the study period; of these, we excluded 425 patients and thus 254 were included in the analysis. The MT group and the no MT group comprised 36 and 218 patients, respectively. Three patients without contrast-enhanced CT scans of the torso, one patient with aortic injury, and two patients with catastrophic brain injury died. However, no patients died due to exsanguination without receiving MT.
The baseline patient characteristics are summarized in Table 1. Patients who required MT presented with significantly higher rates of older age, more severe injury with respect to physiological and anatomical parameters, and higher rates of hemostatic interventions than those without MT. Although no significant differences in CTAV of the IVC in the arterial phase were observed between the two groups, patients in the MT group had significantly higher CTAV at all other sites in both the arterial and portal venous phases than the no MT group.
Interobserver reliability of CTAV measurements
Interobserver reliability was found to be excellent, with intraclass correlation coefficients of 0.995 and 0.984; 0.994 and 0.995; 0.996 and 0.983; 0.993 and 0.968; 0.955 and 0.934; and 0.940 and 0.909 for the CTAVs of the pulmonary artery; ascending aorta; descending aorta; abdominal aorta; femoral artery; and IVC in the arterial and portal venous phases, respectively.
Correlation between enhanced CTAVs of major vessels and clinical parameters on arrival or requirement of RBCs within 24 hours
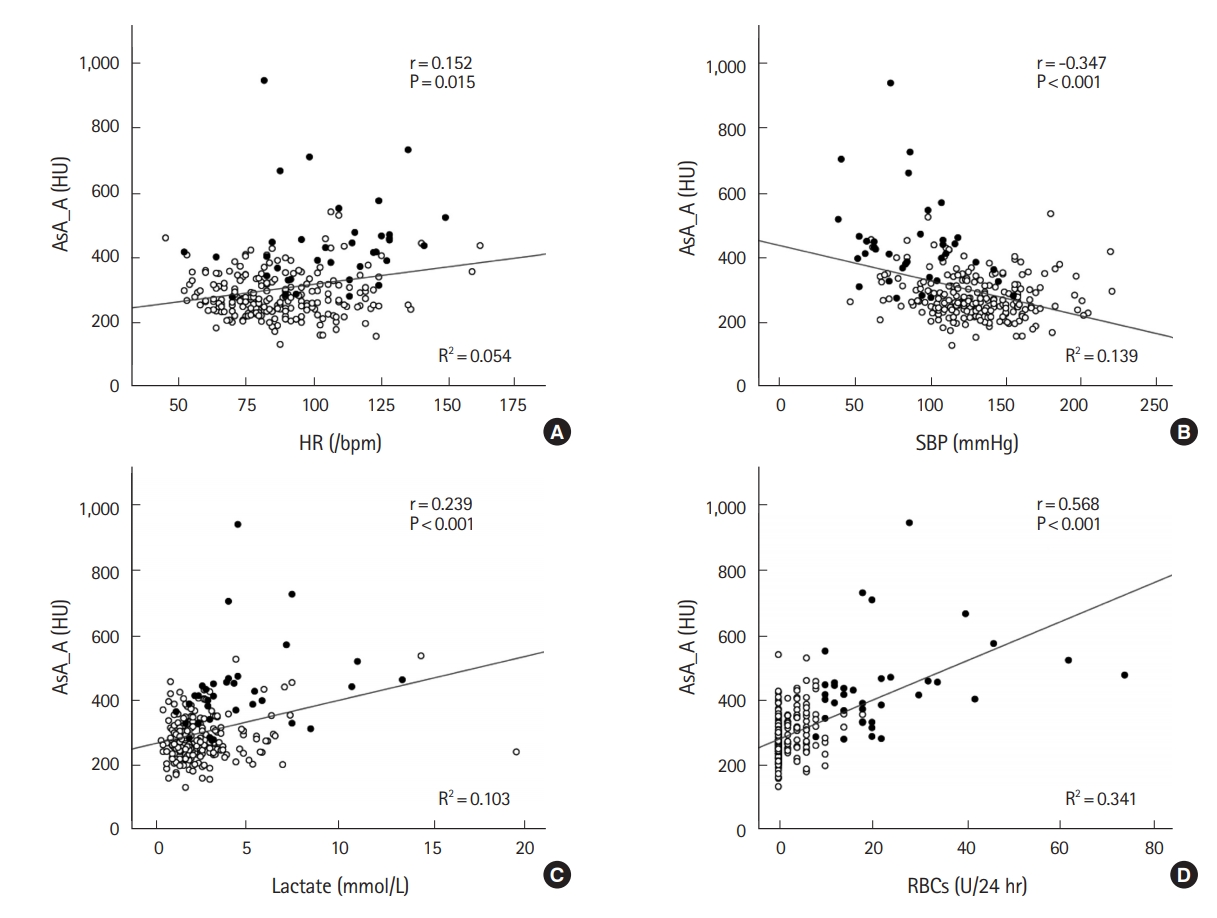
Table 2 shows the correlation between CTAV of major vessels and representative physiological parameters including heart rate, systolic blood pressure (SBP), lactate level on arrival, or requirement of RBCs within 24 hours after arrival. A weak negative correlation was found between SBP and CTAV of all sites in both phases except for IVC in the arterial phase. Meanwhile, a weak positive correlation was observed between lactate level and CTAV of the aorta, except for the ascending aorta in the portal venous phase. RBCs required within 24 hours after arrival were moderately correlated with the CTAV of major vessels in both phases except for the IVC. Fig. 2 shows the correlation between CTAV of the ascending aorta in the arterial phase and the four parameters. CTAV of the ascending aorta in the arterial phase showed the strongest correlation with RBCs required within 24 hours (r=0.568, P<0.001).
Predictive values of enhanced CTAVs for MT
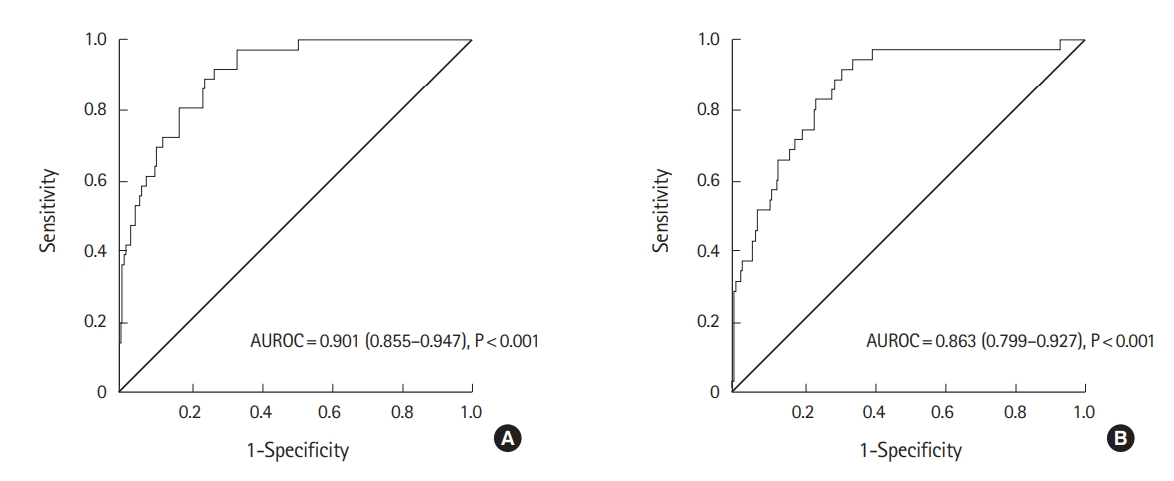
The accuracy of enhanced CTAV of major vessels and other variables as predictors for MT was assessed (Table 3). Enhanced CTAV of major vessels except for the IVC showed moderate accuracy, with an AUROC greater than 0.7. The descending aorta in the arterial phase had the highest accuracy; the AUROC was 0.901 (95% confidence interval [CI], 0.855 to 0.947; P<0.001) (Fig. 3A). The cut-off that maximized the Youden index was 304 HU, with a sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio of 0.889 (95% CI, 0.759 to 0.955), 0.757 (95% CI, 0.735 to 0.768), 3.656 (95% CI, 2.868 to 4.114), and 0.147 (95% CI, 0.058 to 0.328), respectively.
Similarly, the CTAV of major vessels adjusted by the iodine dose per body weight was also confirmed to be a moderate predictor for MT. The ascending aorta in the arterial phase had the highest accuracy; the AUROC was 0.863 (95% CI, 0.799 to 0.927; P<0.001) (Fig. 3B). The cut-off that maximized the Youden index was 0.57 HU*kg/mg, with a sensitivity, specificity, positive likelihood ratio, and negative likelihood ratio of 0.750 (95% CI, 0.603 to 0.859), 0.697 (95% CI, 0.673 to 0.715), 2.477 (95% CI, 1.843 to 3.015), and 0.359 (95% CI, 0.198 to 0.590), respectively.
DISCUSSION
In this study, we found a strong association between initial enhanced CTAV of the aorta and the necessity for MT in major blunt trauma patients. A simple measurement of CTAV of the ascending or descending aorta in the arterial phase, which had the highest interobserver agreement and accuracy, could predict the requirement for MT. A higher CTAV of the aorta should alert the trauma surgeon or emergency physician to activate their MT protocol.
Currently, whole-body CT scanning, which includes a contrast-enhanced scan of the torso, at initial assessment has been suggested to contribute to lower overall mortality than selective CT scanning in trauma patients [23]. A recent study in Japan showed that CT examination was performed in more than 90% of unstable blunt trauma patients during initial management [24]. The whole-body CT scan has become an initial critical diagnostic tool in major trauma patients [25]. Examination at initial assessment is crucial as it can reveal unforeseen bleeding sources and help determine the appropriate hemostatic procedure according to priority [13]. However, despite the widespread use of CT, its findings have not been used to predict the need for MT, except for the presence of intra-abdominal free fluid collection, IVC diameter, or patterns of pelvic ring fracture and the presence of contrast extravasation in the region [9,15,26]. Persistent appearance of a higher density of intravascular contrast material in trauma patients with severe hemorrhage caused us to investigate the association between CTAV and the need for MT.
Enhancement quality of the major vessels is mainly affected by cardiac output and body weight under conditions of a constant protocol [27]. A previous report showed that cardiac output obtained via dynamic CT of the main pulmonary artery correlated well with cardiac output determined using the thermodilution method via right heart catheterization [27]. Another report described a negative correlation between CTAV and cardiac output obtained via echocardiography [28]. Our findings show that higher enhanced CTAV of the aorta in patients who require MT indicates lower cardiac output due to ongoing bleeding. No correlation between CTAV at the IVC in the arterial phase and MT was observed, which was considered as insufficient enhancement of the IVC [29].
In patients with traumatic hypovolemic shock, enhancement patterns of solid abdominal organs have been investigated, and preserved enhancement of the adrenal gland, prolonged enhancement of the pancreas, or decreased enhancement of the renal medulla have been found [16,30]. However, the detailed characteristics of the cohort or variable clinical parameters were unknown, and enhancement patterns varied depending on the severity of shock [30]. Notably, we showed that the lower the SBP and the higher the lactate level on arrival, the more likely the increased enhanced CTAV of the aorta. However, an important limitation must be acknowledged, that is, the clinical parameters and enhanced CTAV of major vessels were not measured simultaneously.
We measured the CTAVs of six major vessel points to examine their predictive capability and reliability. Among them, increased absolute CTAV of the ascending or descending aorta in the arterial phase and its adjusted values according to iodine dose per body weight was revealed to be a highly accurate and reliable predictor of the need for MT. A relatively lower interobserver agreement of CTAV at the IVC may be explained by insufficient mixing of contrast material and vascular collapse due to hypovolemic shock [15,29].
Our study had several limitations. First, the total iodine dose per body weight varied. The body weight and iodine dose administered are the most important factors affecting the magnitude of vascular contrast enhancement [19]. Other affecting factors include the duration of injection and scan delay (i.e., the time interval from the start of contrast material injection to the initiation of scan), which were constant in all patients in the present study [19]. In a clinical trauma care setting, the exact body weight is unavailable. Although the iodine dose was adjusted by estimating body weight, there was no significant difference with respect to total iodine dose per body weight between the MT group and no MT group. Also, the same results were obtained using both absolute CTAV and its values adjusted according to the iodine dose per body weight. Second, institutions use different CT scanners and different dynamic CT protocols, indicating difficulty of generalization, particularly in terms of absolute CTAV. Third, cardiac function, which affects the degree of contrast enhancement, particularly in a patient with heart failure, was not evaluated. Fourth, the time interval between patient arrival to CT scan was not accounted for, which would have been a relevant factor in our study. Finally, our study was a single-center retrospective design. Further large studies are warranted to validate our findings.
In conclusion, initial elevated enhanced CTAV of the aorta is a predictor of the need for MT. Given the high interobserver agreement and AUROC, a simple measurement of CTAV at the ascending or descending aorta in the arterial phase may help in determining the need for MT in patients with major blunt trauma.