Ultrasound-guided regional anesthesia for the pain management of elderly patients with hip fractures in the emergency department
Article information
Abstract
Objective
We examined the pain-relieving effect of ultrasound-guided regional anesthesia performed by emergency physicians on elderly hip fracture patients.
Methods
This study is a prospective, non-randomized, case-control study. The subjects were patients older than 65 years who visited the emergency department with a hip fracture. After we obtained informed consent, two emergency physicians performed an ultrasound-guided three-in-one femoral block using 20 mL of 0.5% bupivacaine. The pain score was measured just before regional anesthesia, and 0.25, 0.5, 1, 2, 3, and 4 hours after the procedure. Another group of patients was given multiple doses of morphine to control the pain. We compared the change in pain score and the development of adverse reactions between the two groups.
Results
A total of 47 patients were enrolled in this study, of which 25 were given regional anesthesia. Successful pain control (pain score<4) was significantly higher in the regional anesthesia group (96.0% vs. 40.9%; P<0.001). The decrease in pain score was significantly higher in the regional anesthesia group (7 [interquartile range, 6 to 7] vs. 4 [interquartile range, 3 to 5]; P< 0.001). The only adverse reaction observed was mild nausea in 4 patients (1 out of 25 from the regional anesthesia group and 3 out of 22 from the morphine group).
Conclusion
Ultrasound-guided regional anesthesia administered by emergency physicians treating elderly hip fracture patients provided faster pain relief and a larger decrease in pain than conventional intravenous injections of morphine.
INTRODUCTION
Hip fractures are common amongst the elderly and can often result in fatal consequences [1]. Proper pain management for acute hip fracture patients can improve patient comfort and reduce complications, morbidity, and mortality [2]. Because most hip fracture patients seek treatment in the emergency department, emergency physicians have an important role in the early management of these patients [3]. However, pain control is often inadequate in the emergency department, particularly when it is overcrowded [4].
Opioid analgesics are used as a first-line drug for acute pain relief [5]. However, they can cause adverse reactions, and the risk of such reactions is particularly higher in the elderly [6]. In order to minimize these adverse reactions, analgesics should be administered using multiple low doses under patient control; however, this results in a large consumption of medical resources. Thus, safely reducing pain to an appropriate level in elderly hip fracture patients in overcrowded emergency departments is a challenging task for emergency medical staff [5,7].
Regional anesthesia is an alternative method of pain control that can replace injection of intravenous opioids in patients with hip fractures [8]. Regional anesthesia alleviates pain in a targeted area of the body, resulting in fewer systemic adverse reactions when compared to intravenous opioid administration. Despite these advantages, regional anesthesia is usually only administered by anesthetists before and after surgery [9]. Recently, it has been shown that regional anesthesia can be carried out more safely under ultrasound guidance, and some studies have reported that it can be used safely in the emergency department [10].
In Korea, local and regional emergency medical centers have a legal requirement to have ultrasound machines. However, no research has been carried out in Korea on regional anesthesia carried out by emergency physicians for hip fracture patients. In the present study, we have examined the success rate of ultrasound-guided regional anesthesia carried out by emergency physicians on elderly patients brought to the emergency department for hip fractures, and have compared the procedure with conventional intravenous morphine administration in terms of the effectiveness of pain relief and the frequency of adverse reactions.
METHODS
Study design
This study is a prospective, non-randomized, case-control study. It was approved by the Institutional Review Board of Hanyang University Guri Hospital (HYGH 2013-P-14).
Study participants
The subjects were 65-year-old or older hip fracture patients who visited the emergency department of a university hospital. The exclusion criteria were as follows: a relatively low pain score (numeric rating scale [NRS], less than 5 out of 10); the presence of accompanying injuries in other parts of the body in addition to a hip fracture; abnormal findings from a nerve/blood vessel examination of the lower limb affected by the hip fracture; difficulty in accurate physical examination or inquiry as a consequence of low consciousness levels or other reasons; and systolic blood pressure below 90 mmHg. We also excluded patients taking anticoagulants, those that had infections of the affected site, those allergic to local anesthetics, those expected to show a change in the anatomical structure of the affected site due to the surgery or procedure.
Study protocol
When an elderly patient aged over 65 years who was suspected of having a hip fracture arrived at the emergency department, inquiry and physical examination were performed initially, and then an intravenous line was established. Saline infusion was started at 100 mL/hr and 5 mg of morphine was administered through slow intravenous infusion for 2 minutes. A definite diagnosis of hip fracture was made using imaging, and if the patient did not meet any of the exclusion criteria, the researcher obtained informed consent for the research from the patient or the guardian and the procedure was performed. An emergency physician performed ultrasound guidance and needle manipulation with an emergency medicine resident’s assistance. None of the practitioners had any previous experience of regional anesthesia before taking part in the study; before participating in the study, they attended a one-hour lecture and practical training provided by a lecturer certified by World Interactive Network Focused on Critical Ultrasound (WINFOCUS). The regional anesthesia method used was three-in-one femoral nerve block [11]. The procedure was performed with monitoring of electrocardiography, blood pressure, and pulse oxygen saturation to anticipate emergency situations. The patient was placed in a supine position with the leg on the affected side in a state of external rotation. The pathways of the femoral vessels, iliacus muscle, and femoral nerve were determined in the emergency department by scanning the region just below the iliac ligament of the affected side using a high-frequency 12-MHz linear probe attached to an ultrasound testing machine (GE Logiq 7, GE Medical Systems, Milwaukee, WI, USA). Then, 20 mL of 0.5% bupivacaine was prepared in a 20 mL syringe as local anesthetic. The injection site was disinfected with chlorhexidine solution and the surrounding region was covered with a sterile cloth leaving only the injection site exposed. The ultrasound transducer was capped with a sterilized plastic cover to prevent infection. Under ultrasound guidance, the skin was punctured with a 21 G spinal needle approximately 2 cm lateral to the femoral artery and both fascia lata and fasica iliaca were penetrated in a succession until the tip of the needle was positioned close to the femoral nerve, after which the local anesthetic was injected around the femoral nerve (Fig. 1) After the injection, pressure was applied to a region approximately 2–4 cm below the puncture site for 5 minutes. We determined the outcome variable as the success of the regional anesthesia. The success of regional anesthesia was defined as the occurrence of dysesthesia in the anterior thigh. In addition, the pain score on a 10-point scale was measured just before regional anesthesia and 0.25, 0.5, 1, 2, 3, and 4 hours after the procedure. After regional anesthesia, the patient was checked for abnormal responses including low blood pressure, vascular perforation, needle damage to the bone, pain at the treated site, dizziness, tinnitus, perioral numbness, and absence of pain relief after 30 minutes. If additional analgesics were required, morphine was administered and the dose was recorded.

Ultrasound-guided three-in-one block method. (A) shows sonoanatomy of right femoral nerve (n), femoral artery (a), and Iliacus muscle (m), and (B) shows puncture site for right femoral nerve block. The linear probe is located just below right inguinal ligament (dot-line).
For patients that did not consent to regional anesthesia or could not undergo the procedure due to the absence of a practitioner, emergency department overcrowding, or any other reason, pain was controlled through intravenous morphine injection. Emergency physicians in charge of the patients in the morphine group were not aware of the study, and controlled pain according to the hospital’s established guidelines. These guidelines include intravenous infusion of 5 mg of morphine over 2 minutes followed by intravenous infusion of 2.5 mg at 10-minute intervals until the appearance of an appropriate analgesic effect. The presence of adverse reactions was checked before each injection and an additional dose was administered only when there was no adverse reaction. The total dose of morphine was decided at the emergency physician’s discretion. For the morphine group, the pain score was measured at 0.25, 0.5, 1, 2, 3, and 4 hours after the first morphine injection and the incidence of adverse reactions was recorded.
Statistical analysis
Statistical analyses were performed using SPSS ver. 18.0 for Mac (IBM Co., Armonk, NY, USA). For the descriptive statistics, nominal variables were expressed as frequency and percentage, ranking-scaled variables as median and quartiles, and ratio-scaled variables as mean and standard deviation. Fisher exact test was used to compare the frequency of adverse reactions between the regional anesthesia group and the morphine group, and t-tests were used to compare the pain scores.
RESULTS
The research period was from January 1 to December 31, 2013. During this period, a total of 145 hip fracture patients aged over 65 years visited the emergency department, and 47 of these were included in the study (25 in the regional anesthesia group and 22 in the morphine group) (Fig. 2). There was no significant difference between the morphine group and regional anesthesia group for gender, age, length of emergency department stay, and initial blood pressure (Table 1).

Flow chart of the study.

General characteristics of subjects according to the analgesia method
Regional anesthesia, judged as dysesthesia of the anterior femur, was successful in all patients in the regional anesthesia group. The initial pain score was 8 (interquartile range [IQR], 7 to 8) for the morphine group and 8 (IQR, 7 to 8.5) for the regional anesthesia group, with no significant difference found between the two groups. However, there was a significant difference in the reduction in pain score (P<0.001); the number of patients whose pain score decreased to less than 4 after the pain treatment was 9 out of 22 (40.9%) in the morphine group, and 24 out of 25 (96.0%)in the regional anesthesia group (Table 2). The magnitude of the decrease in the pain score was also significant (P<0.001); the difference between the initial pain score and the pain score at maximum pain relief was 7 (IQR, 6 to 7) in the regional anesthesia group, and 4 (IQR, 3 to 5) in the morphine group. In the regional anesthesia group, only 1 out of the 25 patients required an additional 5 mg injection of morphine after the procedure. However, in the morphine group, all of the 22 patients required additional morphine injections after the first administration of 5 mg of morphine, and the mean dose of morphine was 11.4±4.9 mg. The only adverse reaction observed was mild nausea in 1 out of 25 patients in the regional anesthesia group. There were no other abnormal symptoms observed. No patient exhibited a 20 mmHg or larger change in systolic or diastolic blood pressure, or any other abnormal findings in vital signs. In the morphine group, nausea was observed in 3 out of 22 patients, but there were no other adverse reactions. No side effects directly associated with the regional anesthesia procedure were observed.
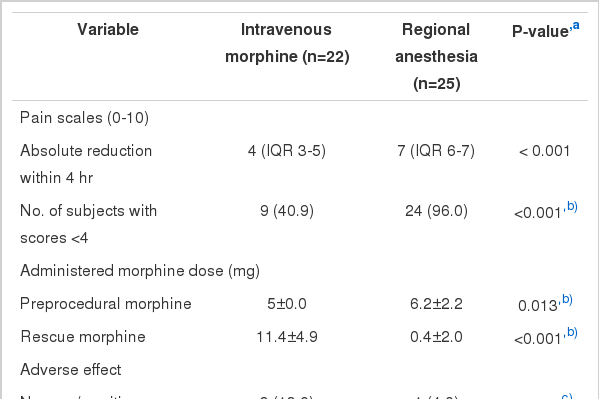
Patients’ outcome by group
Fig. 3 shows the changes in the pain scores for the morphine group and the regional anesthesia group. The decrease in pain score was more rapid and of a greater magnitude in the regional anesthesia group. In the regional anesthesia group, the median pain score decreased to less than 4 in approximately 15 minutes following the procedure. In addition, a low pain score of less than 4 was maintained for more than 4 hours following the procedure in this group. However, in the morphine group, the median pain score did not fall below 4 until 4 hours after the first morphine injection.

The pain scale changes according to the pain management methods. IQR, interquartile range.
DISCUSSION
Inadequate pain management in elderly patients may induce delirium that is known to be associated with a higher mortality rate [12]. In this study, the median pain score of the elderly hip fracture patients was as high as 8 out of 10, and the majority required pain treatment. According to a number of surveys, pain is often not appropriately managed in emergency departments [4]. Bijur et al. [13] reported that the conventionally recommended dose of 0.1 mg/kg of morphine is not sufficient for effective pain control, with additional injections often required. In the elderly population, pain is not always effectively managed because of the fear of potential adverse reactions to opioid analgesics [4]. In this study, the median pain score did not fall below 4 in the morphine group, which suggests that conventional pain treatment with morphine is not adequate. However, the reasons for the use of low-dose opioid analgesics were not assessed in this study. On the other hand, the risk of morphine overdose is a serious consideration in pain management [14]. For safe and effective pain relief, an alternative pain management method that can replace or supplement the intravenous administration of opioid analgesics may be required.
Regional anesthesia is recommended as an alternative or adjuvant method to intravenous opioid analgesic administration for musculoskeletal pain [15]. However, this method is not generally used in emergency departments. According to a recent questionnaire survey of multiple emergency departments in Australia, regional anesthesia was used in only 45 out of 646 hip fracture patients (7.0%) [9]. A recent nationwide survey from the UK reported that only 44% of the emergency departments were using regional anesthesia for hip fracture patients, stating that a lack of trained personnel (36%) and equipment were the major factors [3]. In Korea, we assume that the use of regional anesthesia in emergency departments is low although no survey has been conducted to address this question.
There are two principal regional anesthesia methods that are applicable to pain management in hip fracture patients: fascia iliaca compartment block and three-in-one femoral nerve block. Both can be easily performed on hip fracture patients as a blind technique using anatomical landmarks in the emergency department [16]. In a hip fracture, regional anesthesia can be used to block the lateral femoral cutaneous nerve, the obturator nerve, and the femoral nerve; blocking the latter two nerves produces a pain-relieving effect by cutting off sensation from the femoral neck and reducing the spasm of the quadriceps and the adductor muscle of the thigh. It is known that the combined use of regional anesthesia with intravenous narcotic analgesic infusion is effective in pain relief both before and after hip surgery [17]. In agreement with a previous report, this study has shown that pain reduction achieved using regional anesthesia was more rapid and effective than that achieved using morphine alone. We also found that the need for additional analgesic injections was less common in the group in which regional anesthesia was used following initial morphine administration. Other studies have reported that the time required to achieve the lowest pain score was shorter and the additional dose of opioid analgesics required was lower in emergency hip fracture patients treated with regional anesthesia than in those receiving intravenous analgesics [16].
The use of regional anesthesia employing anatomical landmarks does carry the risk of adverse reactions such as nerve damage and vascular perforation, and it is not easy to prepare nerve stimulants to prevent these side effects. In contrast, ultrasound-guided regional anesthesia performed by monitoring the anatomical region to be anesthetized, can be performed more rapidly and more safely and so may be more suitable for use in the emergency department [18]. When a three-in-one femoral nerve block is applied under ultrasound guidance, the anesthetic is more accurately injected into the desired region enhancing the nerve block effect. As a result, this procedure can achieve the same effect as that of a fascia iliaca compartment block while using a lower dose of anesthetics [19]. We obtained a satisfactory result with an injection of only 20 mL compared to the dose of 30 mL of local anesthetic usually required for a fascia iliaca compartment block.
Some previous studies have reported the use of this procedure in emergency departments, but the procedure was rarely performed by emergency physicians [16]. In this study, emergency physicians without experience in the procedure had approximately one hour of training and then were able to carry out regional anesthesia successfully in all of the 25 patients. This suggests that it is not difficult for inexperienced clinicians to acquire and maintain this skill. Accordingly, we believe that emergency physicians can carry out regional anesthesia quickly and effectively in the emergency department [20].
This study has some limitations. Patients were recruited from only one emergency medical center and the number of subjects was relatively small. Only two practitioners performed regional anesthesia so its effect may have been overestimated and the incidence of complications may have been underestimated. This was not a randomized blinded study so there could be a selection bias. The dose of morphine used in the morphine group may not have been high enough to control pain; morphine was administered at the attending physician’s discretion and the researcher did not intervene in the process of pain management; the incidence of adverse reactions might have been higher in the morphine group if an adequate dose had been administered. As a consequence, adverse effects in the regional anesthesia and morphine groups may not be directly comparable. Nonetheless, the regional anesthesia group showed satisfactory pain relief within a relatively short time, and apart from one case, did not require additional analgesic injections. Thus, this study is meaningful in that it indicates that the combined use of regional anesthesia with initial morphine administration in the emergency department by emergency physicians can be more effective and safer for pain control than the administration of opioid analgesics only. The dose of preprocedural morphine was significantly higher in the regional anesthesia group. However, only 2 patients in the regional anesthesia group were given more than 5 mg of morphine and their total dose was less than 10 mg; therefore, it is unlikely that this had a significant effect on the results.
In conclusions, ultrasound-guided regional anesthesia performed by emergency physicians for hip fractures in elderly patients showed a high success rate without any serious adverse reactions. In addition, it produced more rapid and effective pain relief than conventional intravenous morphine injection therapy. The results of this study suggest that the combined use of ultrasound-guided regional anesthesia and intravenous opioid analgesic administration in elderly patients with hip fractures, in an emergency department setting, can provide faster, safer, and more effective pain relief than currently used methods.
Notes
No potential conflict of interest relevant to this article was reported.
References
Article information Continued
Notes
Capsule Summary
What is already known
Regional anesthesia may be an alternative method of pain control to replace injection of intravenous opioid in patient with hip fracture. However, regional anesthesia for hip fracture patients have been applied usually by anesthesiologists just before and after surgery.
What is new in the current study
Emergency physician can safely and correctly perform regional anesthesia for elderly hip fracture patients using ultrasound guidance.