Emergency medical service personnel need to improve knowledge and attitude regarding prehospital sepsis care
Article information
Abstract
Objective
We aimed to evaluate the knowledge and attitudes of emergency medical service (EMS) personnel pertaining to sepsis. We also compared EMS personnel’s knowledge of sepsis and their intention to engage in prehospital sepsis management.
Methods
The survey was conducted during education conferences for EMS personnel in December 2013 and January 2015 in Seoul, Korea. The questionnaire composed of 10 questions relevant to sepsis, was distributed on-scene, and was retrieved by investigators after the conference. We classified subjects into active and passive groups based on intent to participate in prehospital sepsis care.
Results
A total of 271 questionnaires were distributed; 255 EMS personnel (94%) completed the survey, 126 (49%) of whom were first-degree emergency medical technicians (EMTs). Less than 75% of subjects provided clinically relevant responses to questions about the definitions of sepsis, tachycardia, tachypnea, hypotension, hypothermia, fluid resuscitation, and vasopressor. Only 15% of participants had suspected that a patient had sepsis, and 9% reported that they could identify patients with sepsis during transportation. Overall, first-degree EMTs showed higher levels of knowledge and a positive attitude to sepsis compared with non-first-degree EMTs. Sixty percent of the participants reported that they were actively involved in prehospital sepsis care. The active group showed significantly higher levels of knowledge and more positive responses to the clinical impact of prehospital sepsis care.
Conclusion
Our study showed that is a substantial portion of EMS personnel lacks appropriate level of knowledge on sepsis care. We also found that the intention to engage in sepsis management was associated with appropriate knowledge of sepsis.
INTRODUCTION
Sepsis is a leading cause of death worldwide, and the incidence of sepsis has increased over the past decades due, in part, to increasing age and chronic illness [1,2]. Like acute myocardial infarction and cardiac arrest, sepsis is time-sensitive. It is clear that early recognition and timely management of sepsis improve patient outcome [3-6].
Approximately 30% to 50% of patients with sepsis are transported to the emergency department (ED) by emergency medical service (EMS) [7-10]. It implies that the prognosis of these patients would be influenced by prehospital care performed by EMS personnel [11]. As EMS personnel might be the first health care providers for patients with sepsis, they are very important in initiating the cascade of sepsis care before hospital arrival. To provide optimal sepsis care in a prehospital setting, EMS personnel should be familiar with the disease and proactively involved in sepsis care. However, understanding of sepsis among EMS personnel might be insufficient, which can negatively impact their attitude and performance [12].
We conducted this survey to evaluate the knowledge and attitudes of EMS personnel regarding sepsis care and to compare their understanding about sepsis based on willingness to be involved in prehospital sepsis care.
METHODS
Study design and data collection
The survey was conducted during education conferences for EMS personnel in December 2013 and January 2015 in Seoul, South Korea. Our subjects were EMS personnel who work at the fire stations in a metropolitan city [13].
The questionnaire was composed of 10 sepsis-related questions and was developed based on previous survey studies (Appendix 1) [14]. The survey was designed to assess basic knowledge of the diagnosis and treatment of sepsis, as well as the attitude toward managing sepsis patients in a prehospital setting. A questionnaire was distributed to all participants at the beginning of the conference. They were asked to complete the questionnaire during the conference, and it was later retrieved by investigators.
The institutional review board of our institute approved this study, and written informed consent was obtained from each participant before performing the survey. No incentives were offered for participation in the survey.
Study population
EMS personnel in South Korea are categorized into first-degree emergency medical technicians (EMTs), second-degree EMTs, and drivers. Based on their medical roles and certification, these are analogous to EMT-intermediate, EMT-basic, and first responder, respectively, in the US EMS system. First-degree EMT is the highest level of EMT certification, and these subjects undergo at least three years of training at a vocational college. They are certified to perform advanced cardiopulmonary life support including endotracheal intubation, intravenous access, and administration of limited rescue drugs under the on-line medical directions by physicians. First-degree EMTs also perform all of the same functions as second-degree EMTs and drivers. Second-degree EMTs and drivers are usually trained at fire departments or other certified facilities. Their performance is limited to basic cardiopulmonary life support, wound management, and patient assessment. Most ambulances are staffed by one or two EMTs (first-degree EMT and/or second-degree EMT) and a driver.
Data analysis
We classified participants into first-degree EMT group and non-first-degree EMT group (second-degree EMT and driver) for data analysis. We also classified EMS personnel into active and passive groups according to their participatory intentions in prehospital sepsis care. The active group was defined as EMS personnel who answered ‘yes’ to question 10 (are you willing to be actively engaged in the management of sepsis in the prehospital setting?). The passive group was composed of subjects who answered ‘no or not sure’ to this same question. Knowledge and perception were considered insufficient when subjects responded to <75% of the questions appropriately.
Data are presented as mean with standard deviation for numerical data and number with percentage for categorical data. The Students t-test was used for continuous variables, and the chi-square test was used for categorical variables. A P-value less than 0.05 was considered significant. STATA ver. 12.0 (STATA Corporation, College Station, TX, USA) was used for statistical analysis.
RESULTS
Baseline characteristics
A total of 271 questionnaires were distributed, and 255 EMS personnel (94%) completed the survey by the end of the conference. Of the eligible participants, 126 (49%) were first-degree EMTs. Baseline characteristics of each group including age, gender, and EMS career duration are described in Table 1. The mean age of the participants was 34 years, and 219 (86%) participants were men.
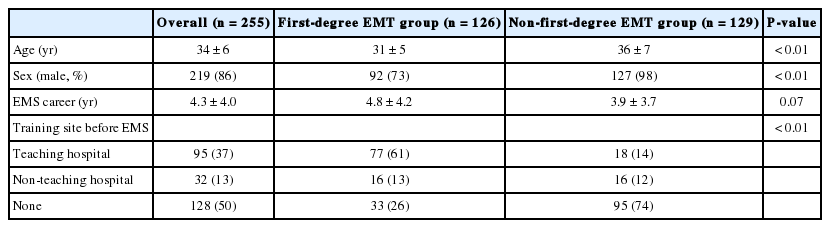
Baseline characteristics
Knowledge and perception of sepsis
Of the 255 participants, 242 (95%) were aware of the term “sepsis” (Q1 in Table 2). Only 171 (67%) participants, however, correctly defined sepsis (Q2) (75% in the first-degree EMT group vs. 59% in the non-first-degree EMT group, P<0.01). First-degree EMTs better understood common signs, symptoms, and treatment options for sepsis than did non-first-degree EMTs. In total, 223 (87%) participants noted that fever was the most frequent symptom of sepsis, followed by altered mental status (78%) (Q3). Relatively few subjects had sufficient knowledge regarding tachycardia (73%), tachypnea (68%), hypotension (49%), and hypothermia (20%).

Knowledge and perception of sepsis
Most of the group was aware of the importance of antibiotics (78%), while fluid resuscitation (61%) and vasopressors in shock (35%) were less frequently considered as essential therapeutic measures (Q4). Only 38 (15%) participants had suspected sepsis in a patient during transportation (26% and 4% of participants in the first-degree EMT group and the non-first-degree EMT group, respectively) (Q5).
Attitude toward prehospital sepsis care
Only 9% of subjects reported that they could identify patients with sepsis during transportation (Q6 in Table 3). More than half of the participants (59%) agreed that EMS personnel should be involved in prehospital sepsis care (Q7). Sixty-three percent responded that their intervention would improve the outcome of patients with sepsis (Q8), and 58% responded that their intervention would positively influence the behavior of the medical team in the ED (Q9).

Attitudes toward sepsis
Of the participants, 154 (60%) were actively willing to be involved in prehospital sepsis care, while 101 (40%) subjects responded in a passive manner (Q10). There was a significant difference between the first-degree EMT group and the non-first-degree EMT group with regard to willingness to be involved in prehospital sepsis care (75% vs. 46%, P<0.01).
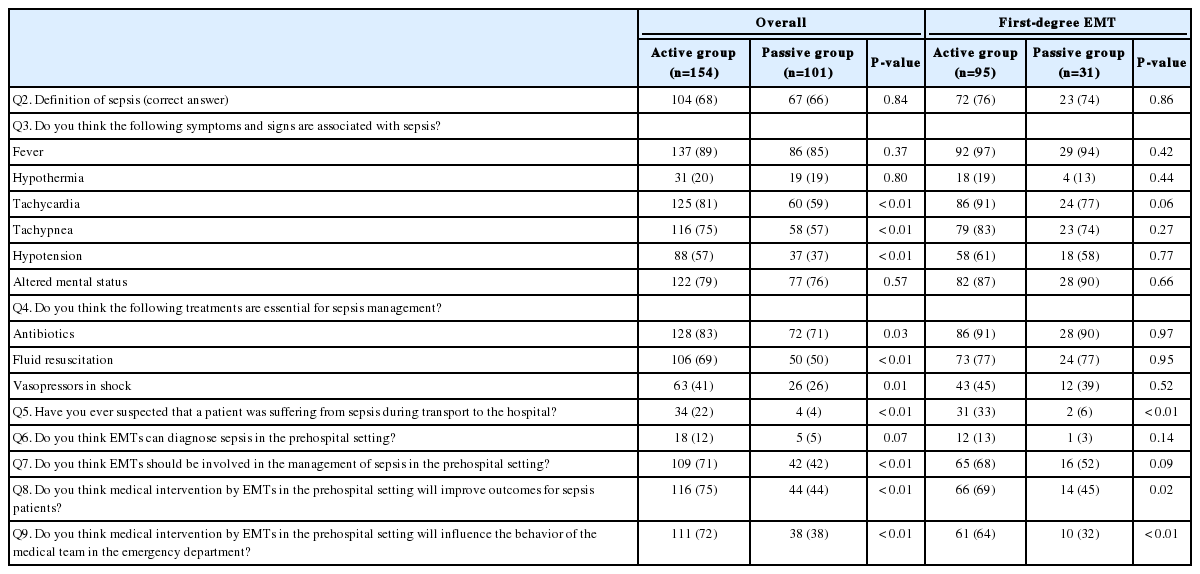
The active group vs. the passive group
Overall, the active group had better knowledge of sepsis than the passive group, and the differences were statistically significant in responses to Q3 (81% vs. 59% for tachycardia, 75% vs. 57% for tachypnea, and 57% vs. 37% for hypotension) and Q4 (83% vs. 71% for antibiotics, 69% vs. 50% for fluid resuscitation, and 41% vs. 26% for vasopressors in shock) (Table 4). The proportion who had ever suspected sepsis in a patient during transportation was significantly higher in the active group (22% vs. 4% overall and 33% vs. 6% in the first-degree EMT group) (Q5). The active group showed a significantly more positive attitude towards prehospital sepsis care, as seen in Q7 (71% vs. 42%), Q8 (75% vs. 44%), and Q9 (72% vs. 38%). The trends between the active and the passive groups were less prominent in the first-degree EMT group.
Comparison of knowledge and attitudes according to activeness of emergency medical service personnel
DISCUSSION
The EMS system has contributed to an improvement in the outcomes of several time-critical diseases in the prehospital setting, such as acute myocardial infarction and cardiac arrest [15,16]. Sepsis is similar and requires immediate intervention [17]. Previous studies have shown that a significant proportion of patients with sepsis were transported by the EMS system [7-10]. Therefore, EMS personnel have crucial roles in early identification of sepsis, timely initiation of elements of treatment, and transporting patients to the appropriate hospital.
We found a lack of knowledge and perception of sepsis among EMS personnel in Korea, in terms of definition, clinical signs, symptoms, and treatment options. EMS personnel who expressed their intention to actively participate in prehospital sepsis care had a better understanding of sepsis and a more positive attitude toward prehospital care for sepsis patients. However, the 40% of EMS personnel who were only passively willing to be involved in sepsis care had lower levels of knowledge and awareness for sepsis. They also had negative impressions of the clinical roles of EMS in sepsis care. These findings suggest a need for improved understanding of sepsis and encouraged involvement by providing education about sepsis and current evidence about prehospital sepsis care.
Our study suggested that lack of knowledge was not the only barrier to care; some subjects had difficulty implementing their knowledge, considering that very few EMTs had ever suspected their patients were suffering from sepsis. Recognizing sepsis is a key step to initiating appropriate care, but it is very challenging in the prehospital setting due to limited clinical information [18]. For EMS personnel, a feasible prehospital protocol to enhance early diagnosis and management is needed. For example, use of systematic screening tools and an on-scene point-of care lactate test might help EMS personnel to identify severe sepsis in the prehospital setting.
Early recognition of sepsis by prehospital personnel should lead to transport of patients to the proper hospital and behavioral changes in hospital staff [19]. More than half of the EMS personnel (58%) agreed that their medical intervention would positively influence the behavior of in-hospital staff. This tendency was remarkably stronger in the active group compared to the passive group. Studnek et al. [7] confirmed that ED arrival by EMS triggered the in-hospital cascade of sepsis care, resulting in a shorter time to initiation of antibiotics and early goal-directed therapy in patients with severe sepsis.
Prehospital sepsis care has not been a subject of intense interest for several decades. Although Seymour et al. [11] showed that prehospital fluid administration and placement of intravenous access decreased hospital mortality compared to no intervention, the importance of prehospital sepsis care and the ability of EMS personnel to improve sepsis outcomes are unknown. Further research is needed to establish clear roles of EMS personnel in sepsis care before hospital arrival.
This study has several limitations. First, the study was carried out during educational conferences for EMS personnel working in a metropolitan city. Therefore, our findings might not be generalizable to other settings such as the rural EMS system. Second, the participant number was relatively small, although the number of first-degree EMTs in this study was approximately 25% of all first-degree EMTs working at Seoul Metropolitan Fire & Disaster Headquarters at the time of the survey [13]. Third, these participants had relatively short EMS career durations compared to participants in previous studies [14], which could have influenced the results.
In conclusion, appropriate knowledge and perceptions regarding sepsis care were insufficient among EMS personnel in Korea. EMS personnel who were actively willing to be involved in sepsis care before hospital arrival showed better knowledge and perception of sepsis compared to those who did not. To reinforce the survival chain of sepsis from the prehospital setting, targeted education for EMS personnel and systematic implementation of a feasible protocol to enhance early management of sepsis will be needed.
Notes
No potential conflict of interest relevant to this article was reported.
References
Appendices
Appendix 1. Questionnaire
Baseline characteristics
1. Age ( )
2. Gender
A. Male
B. Female
3. Emergency medical service (EMS) career duration
4. Emergency medical technician (EMT) grade
A. First-degree EMT
B. Non-first-degree EMT
5. Training site before working in EMS
A. Teaching hospital
B. Non-teaching hospital
C. Not trained
Questions
1. Have you ever heard of the term “sepsis”?
A. Yes
B. No
2. Which one do you think is the most appropriate definition of sepsis?
A. Blood contamination by dirty materials
B. Life-threatening food poisoning after ingestion of seafood such as fish and shellfish
C. Life-threatening infectious disease caused by multidrug-resistant bacteria
D. Systemic inflammatory response caused by microbial infection
E. Allergic reaction against microbes
3. Do you think the following symptoms and signs are associated with sepsis?
A. Fever
i. Yes
ii.No or not sure
B. Hypothermia
i. Yes
ii.No or not sure
C. Tachycardia
i. Yes
ii.No or not sure
D. Tachypnea
i. Yes
ii.No or not sure
E. Hypotension
i. Yes
ii.No or not sure
F. Altered mental status
i. Yes
ii.No or not sure
4. Do you think the following treatments are essential for sepsis management?
A. Antibiotics
i. Yes
ii.No or not sure
B. Fluid resuscitation
i. Yes
ii.No or not sure
C. Vasopressors in shock
i. Yes
ii.No or not sure
5. Have you ever suspected that a patient was suffering from sepsis during transport to the hospital?
A. Yes
B. No or not sure
6. Do you think emergency medical technicians can diagnose sepsis in the prehospital setting?
A. Yes
B. No or not sure
7. Do you think EMTs should be involved in the management of sepsis in the prehospital setting?
A. Yes
B. No or not sure
8. Do you think medical intervention by EMTs in the prehospital setting will improve outcomes for sepsis patients?
A. Yes
B. No or not sure
9. Do you think medical intervention by EMTs in the prehospital setting will influence the behavior of the medical team in the emergency department?
A. Yes
B. No or not sure
10. Are you willing to be actively engaged in the management of sepsis in the prehospital setting?
A. Yes
B. No or not sure
Article information Continued
Notes
Capsule Summary
What is already known
Sepsis is common and treatment is time-critical. However, the knowledge and attitudes of prehospital personnel regarding sepsis are unknown.
What is new in the current study
There is a lack of knowledge regarding sepsis and its management among prehospital personnel in Korea.