Discharge from the emergency department and early hospital revaluation in patients with COVID-19 pneumonia: a prospective study
Article information

Abstract
Objective
The national health systems are currently facing the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. We assessed the efficacy of outpatient management for patients with SARS-CoV-2 related pneumonia at risk of progression after discharge from the emergency department.
Methods
This was a single-center prospective study. We enrolled patients with confirmed SARS-CoV-2 pneumonia, without hypoxemic respiratory failure, and at least one of the following: age ≥65 years or the presence of relevant comorbidities or pneumonia extension >25% on high resolution computed tomography. Patients with pneumonia extension >50% were excluded. An ambulatory visit was performed after at least 48 hours, when patients were either discharged, admitted, or deferred for a further visit. As a control, we evaluated a comparable historical cohort of hospitalized patients.
Results
A total of 84 patients were enrolled (51 male patients; mean age, 62.8 years). Two-thirds of the patients had at least one comorbidity and 41.6% had a lung involvement >25% on high resolution computed tomography; the mean duration of symptoms was 8.0±3.0 days, and the mean PaO2/FiO2 ratio was 357.5±38.6. At the end of the follow-up period, 69 patients had been discharged, and 15 were hospitalized (mean stay of 6 days). Older age and higher National Early Warning Score 2 were significant predictors of hospitalization at the first follow-up visit. One hospitalized patient died of septic shock. In the control group, the mean hospital stay was 8 days.
Conclusion
Adopting a “discharge and early revaluation” strategy appears to be safe, feasible, and may optimize hospital resources during the SARS-CoV-2 pandemic.
INTRODUCTION
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified in December of 2019 in China [1], where it caused the first cluster of cases which was then rapidly transmitted worldwide, leading to a pandemic. This country was overwhelmed, especially early in the pandemic, with more than 4.15 million overall cases and a case fatality rate peak of 6.6%, in the first wave alone [2]. The National Health System of this country, as in most countries, has struggled to withstand the epidemic wave, especially due to a lack of hospital beds, both for ordinary as well as intensive care patients.
Notably, one large epidemiological study found that only 19% of patients with the SARS-CoV-2 infection developed severe or critical illness and pneumonia with hypoxemic respiratory failure as the more frequent complication [3]. While several risk scores designed to help with the management of patients affected by coronavirus disease 2019 (COVID-19) that adopt clinical, radiological, and laboratory markers of progression of the disease have been proposed [4,5]. their real-life applicability is limited, as they must be integrated into a more complex clinical judgment.
Indeed, being discharged from the emergency department (ED) is a crucial moment for these patients’ management. In fact, in a retrospective cohort of low-risk patients (median age of 38 years and 61% without comorbidities) with COVID-19 like symptoms discharged from the ED, the readmission rate was 4% after a median of 5 days [6]. Furthermore, in a multicenter study enrolling only confirmed COVID-19 patients, they found that only about 5% of the patients discharged from the ED returned within 72 hours and were hospitalized (8.2% within 7 days), with the major predictors of readmission being the presence of hypoxia, fever, and age > 60 years [7].
A useful solution for the optimization of resources may be to treat and follow-up these patients as outpatients. Two recent studies in Spanish cohorts during the first pandemic wave reported similar experiences of outpatient management in mild COVID-19 patients, describing a hospitalization rate ranging from 6.2% to 6.4% [8,9].
Therefore, we aimed to identify symptomatic patients with mild-to-moderate COVID-19 pneumonia at their first access to the ED that can be managed at home in order to reserve them a fast-track access to hospital care, if needed, after a continuous medical ambulatory evaluation. The main objective of this study was to evaluate the feasibility and safety of our protocol in patients with SARS-CoV-2 related pneumonia discharged from the ED at risk of progression.
METHODS
Study design, setting, and population selection
The study population consisted of a cohort of patients presented and discharged from our ED and re-evaluated in our COVID-19 early medical revaluation unit, from November 15, 2020 to January 10, 2021. All patients were aged 18 or older and provided written informed consent. The inclusion criteria were (1) confirmed SARS-CoV-2 infection by a real-time reverse transcription polymerase chain reaction nasopharyngeal swab; (2) age ≥ 65 years or presence of at least one comorbidity including hypertension, chronic obstructive pulmonary disease, chronic heart failure, obesity (body mass index > 30 kg/m2), active neoplasia, or semiquantitative pneumonia involvement > 25% on high resolution computed tomography (HRCT); (3) HRCT radiological evidence of interstitial pneumonia with semiquantitative extension ≤ 50% [10] ; and (4) absence of functional respiratory failure defined by the presence of both PaO2/FiO2 ≥ 300 and no desaturation during a quick walking test (QWT) [11]. The patients who did not meet all the inclusion criteria were excluded.
As a control group, we collected clinical data of a historical cohort of patients admitted to the same hospital from March 10 to December 31, 2020 for COVID-19 related pneumonia. Controls were matched at admission to the ED for age, sex, number of comorbidities, evidence of pneumonia on HRCT, and absence of respiratory failure (considered as PaO2/FiO2 ratio > 300).
The local ethics committee waived approval of the study given that our outpatient service was active during the pandemic. The study was performed according to the ethical guidelines of the Declaration of Helsinki (seventh revision). This report is according to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement for observational studies.
Interventions and measurements
Upon discharge, clinicians gave a pulse oximeter and a personal diary to each patient that were asked to measure and report the following results three times daily: body temperature, peripheral oxygen saturation at rest, and after a QWT. Warning signs observed in patients’ diaries were defined as a persistent fever > 38.5°C (detected in at least three consecutive measurements) or a pulse oximetry reading lower than 92% at rest or lower than 90% after a QWT. The COVID-19 early medical revaluation unit was composed of two clinicians (one internist and one emergency physician) and one nurse. The follow-up visit was performed at least 48 hours after discharge and included: a complete physical examination, National Early Warning Score (NEWS2) score, a personal diary check, a standard lung ultrasound examination [12], an arterial blood gas test, and a QWT. After the visit, patients were either discharged, admitted, or referred for a further visit, upon clinical judgment. The last follow-up consisted of a phone call made 30 days after the index admission that considered the patient’s overall satisfaction on a 1 (low) to 10 (high) point scale.
Data analysis
The continuous variables are summarized as mean ± standard deviation. Categorical data are summarized as absolute numbers and percentages. The results were tested for normality using the Kolmogorov-Smirnov test. A Student t-test was used to compare the continuous variables among the subgroups of patients. A chi-square test was used to compare the categorical variables. A logistic regression model was performed to identify variables associated with hospitalization. A P-value < 0.05 was considered significant. All statistical analyses were performed with Stata ver. 14.0 (StataCorp., College Station, TX, USA).
RESULTS
Characteristics of study subjects
In total, 84 patients were enrolled in this study (51 male patients [60.7%]; mean age, 62.8 ± 12.0 years). Table 1 summarizes the baseline characteristics of the cohort. Most patients had one or more comorbidities (22.6% were obese, 23.8% had diabetes, 32.1% hypertension, and 8.3% chronic obstructive pulmonary disease). At admission, the mean duration of symptoms attributable to SARS-CoV-2 infection was 8.0 ± 3.0 days. The most commonly reported symptoms were fever (96.4%), cough (58.3%), shortness of breath (34.5%), fatigue (23.8%), anosmia/ageusia (13.1%), and gastrointestinal symptoms such as nausea, vomiting, or diarrhea (20.2%). The mean peripheral oxygen saturation was 96.8 ± 1.5%, the mean respiratory rate was 16.3 ± 1.8 per minute, and the mean PaO2/FiO2 ratio was 357.5 ± 38.6. Notably, a significant proportion of patients had a lung involvement of > 25% assessed by HRCT (41.7%). All patients were discharged after a mean ED stay of 16.3 ± 14.6 hours, with the above-mentioned instructions and a scheduled follow-up visit.

Baseline characteristics of the enrolled patients (n=84)
Main results
In total, 6 patients (7.1%) were re-hospitalized before the planned visit (five male; mean age, 67.6 ± 9.04 years) after a mean of 1.3 ± 0.5 days at home (Fig. 1). Of the 78 patients that attended the first follow-up visit after a mean of 3.3 ± 1.1 days from the index admission, only one had to start oxygen support at home (prescribed by their family physician). The average peripheral oxygen saturation was 96.6 ± 1.8%, the average respiratory rate was 16.5 ± 3.7 per minute, and the mean PaO2/FiO2 ratio was 375.3 ± 55.1. Notably, most of the patients were receiving a prophylactic dosage of subcutaneous heparin (82.0%) and oral steroids (74.3%). The majority of patients filled out the diaries (88.4%), but warning signs were only noted in 13 of 69 diaries (18.8%). Among 78 patients, four (5.1%) were admitted, 23 (29.5%) were referred for another follow-up visit, and 51 (65.4%) were discharged from hospital care. Of the 23 patients that had been referred for a second visit, four (17.4%) had to be admitted before the planned average follow-up of 4.5 ± 1.9 days. Of the 19 patients that attended the second visit after a mean of 7.4 ± 2.3 days from the index admission, only two (10.5%) needed oxygen supplementation at home. The majority of patients remained on heparin (73.7%) and steroids (68.4%). At the end of the hospital evaluation, among 19 patients, 14 (73.7%) were discharged, one was admitted for persistent fever, and four were further referred for another follow-up visit. Of the 19 patients that were managed in more than one follow-up visit, 14 showed a reduction trend or, at least, displayed a stationary lung ultrasonographic score. All of the patients were finally discharged after the third hospital visit. The mean duration of the ambulatory management was 4.6 ± 2.7 days. The details of the management of the single patients are summarized in Fig. 2.

A flow-chart summarizing the management course of the enrolled patients: admission, revaluation, or discharge.
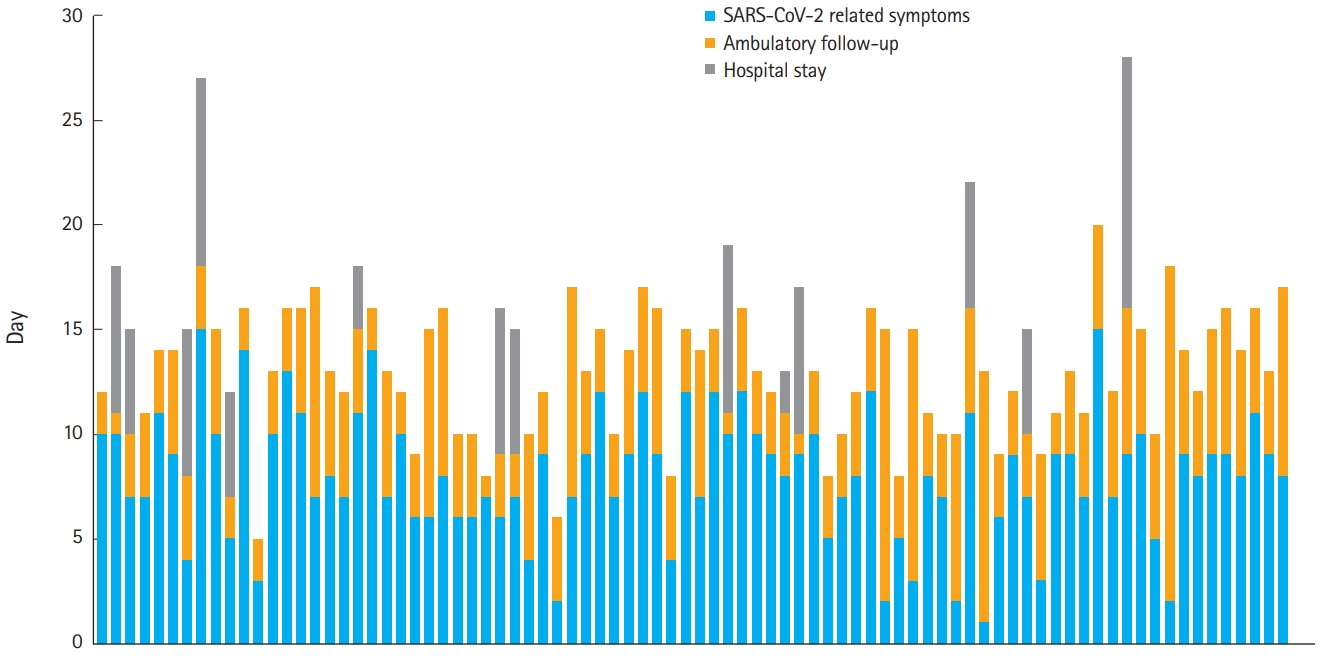
A graph showing the disease course of each patient from the onset of symptoms to discharge or hospitalization. SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
At the 30-day follow-up call, all but one patient were alive. The deceased patient was an 84-year-old woman hospitalized after her second visit because of hypoxemic respiratory failure. After a hospitalization that lasted 12 days (6 in the intensive care unit and 6 in the sub-intensive care unit), she was discharged home. Two days later, she was referred to the ED for fever, chills, myalgias, and shortness of breath. The tests showed the presence of Enterococcus faecium in her urine and Acinetobacter baumannii in her lower respiratory tract. She died of septic shock 36 hours later.
In total, 15 of 84 patients (17.8%) had been admitted by the end of the follow-up window. The mean duration of hospitalization was 6.1 ± 2.5 days. All but three admitted patients (one still receiving low flow oxygen supplementation) were at home at the time of the phone call. The 66 patients that could answer were also asked to rate their satisfaction with their ambulatory service on a 10-point scale. Overall, they rated the service with a mean of 9.1 ± 1.5 points.
Table 2 summarizes the comparisons between patients that were hospitalized and those that were managed at home, considering the variables at the index admission and at the first followup visit. Overall, there were no differences between the two groups at the index admission except for age (higher for the hospitalized group). Conversely, considering only patients that attended the first follow-up visit (n = 78), the hospitalized group showed a higher mean NEWS2, lower peripheral oxygen saturation at rest and after a walking test, a lower PaO2/FiO2 ratio, and more importantly, their diary was more likely to be positive for warning signs while at home.
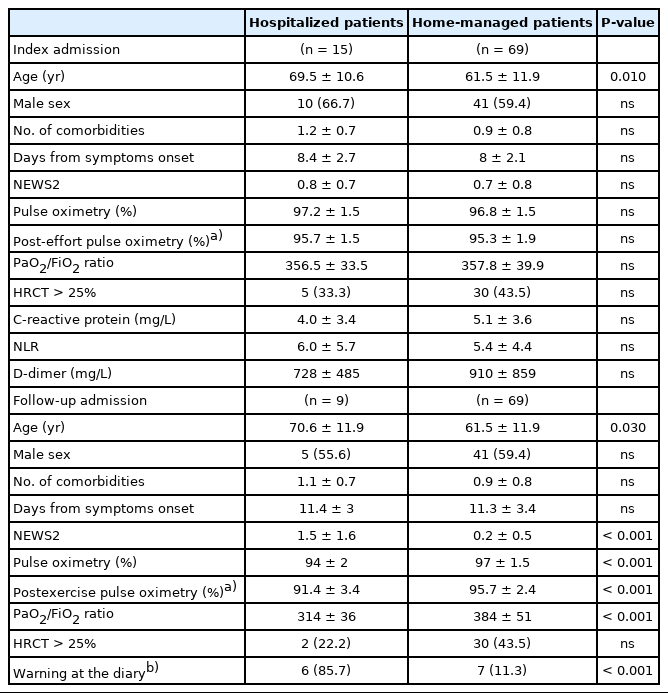
Difference between patients that have been hospitalized or patients managed at home, at the index admission (n=84) or the first follow-up admission (n=78)
None of the variables in the univariate analysis were significant predictors of hospitalization within the follow-up period at the index of ED admission, except for age (odds ratio [OR], 1.06; 95% confidence interval [CI], 1.01–1.11). Considering the first follow-up visit, age (OR, 1.11; 95% CI, 1.00–1.23), and NEWS2 (OR, 7.76; 95% CI, 1.66–36.1) were significant predictors of hospitalization after adjusting for confounding factors (Table 3). Of the 10 patients admitted by the end of the first scheduled follow-up, only two had a NEWS2 score ≥ 2 at the index admission (suggesting a disease progression), whereas all four of the patients that presented to the first visit with a NEWS2 score ≥ 2 were hospitalized.

Results of the logistic regression model: predictors of hospital admission at the first follow-up visit (n=78)
Next, we compared the group of patients that were managed with the early discharge and re-evaluation protocol with that of a historical cohort of patients that presented to our ED and was hospitalized and was matched for age, sex, number of comorbidities, evidence of pneumonia on HRCT, and absence of respiratory failure (considered as PaO2/FiO2 ratio > 300). The cohorts were substantially comparable for the main variables (Table 4).

Differences between enrolled patients and an historical cohort of patients, matched for age, sex, number of comorbidities, and absence of respiratory failure
Although the mean duration of hospitalization was not different between the groups (6.2 ± 5.5 vs. 8.8 ± 5.2 days), we found that only 15 of 84 patients (17.8%) were hospitalized, compared to 63 patients in the historical cohort.
DISCUSSION
Discharging SARS-CoV-2 pneumonia patients without hypoxia from the ED and managing them in an ambulatory service appears to be safe and feasible. Of the 84 enrolled patients, all of them completed the follow-up. Only one patient died of septic shock due to a nosocomial infection after hospitalization was needed for the progressive development of hypoxia detected in a control visit. Notably, this cohort of patients is representative of those with SARS-CoV-2 related pneumonia who are at low-to-moderate risk for progression of the disease [4,13], as 60.7% of them were male, the mean age was 62.8 years, with one or more comorbidities, and 41.6% of them had a lung involvement higher than 25% (but lower than 50%) based on their HRCT score. Fever was reported by almost all of the patients (96.4%), the presence of a cough by more than a half (58.3%), and shortness of breath by a third of them (34.5%).
Importantly, COVID-19 has a triphasic course: the early disease (I), the pulmonary (IIa, without and IIb, with hypoxia), and the hyperinflammation phases [14]. With the ambulatory strategy, we tried to reevaluate patients between stage IIa and IIb. In fact, our patients complained of symptoms attributable to SARS-CoV-2 infection starting on day 8.0 ± 3.0 days with a mean duration of ambulatory management of 4.6 ± 2.7 days.
At the index admission, the respiratory status of all the patients was satisfactory, as they were eupneic, with a negative QWT, and their PaO2/FiO2 ratio was at the lower boundaries required for oxygen supplementation. Older age and higher NEWS2 appear to be the most important predictors of hospitalization. Notably, a previous small prospective Norwegian study found that the NEWS2 score predicted severe disease and in-hospital mortality better than the other risk scores evaluated [15]. However, a larger multi-centered cohort found that the model of ‘NEWS2+age’ alone had poor-to-moderate discrimination for severe COVID-19 at 14 days (area under the curve, AUC 0.7), which could be improved with the integration of other blood and physical parameters [16]. These limitations aside, this is the first study to assess the utility of a longitudinal evaluation of NEWS2 score for outpatients with COVID-19.
Importantly, a high proportion of patients filled out the diary suggesting satisfactory training during the enrollment as well as good performance status and/or correct engagement of the caregiver. This tool proved to be useful and helped the physicians during the follow-up visit decide how to manage their patients. Notably, in our cohort, 85.7% of the patients hospitalized after a control visit had warning signs in their diary, versus the 11.3% that were not hospitalized. Furthermore, for COVID-19 patients, the presence of a caregiver or social support is crucial due to the risk of progression; in our cohort, the lack of home assistance represented the reason for hospitalization in two out of 15 patients.
Unsurprisingly, there was no difference between the patients managed at home and those hospitalized with regard to lung involvement as assessed by HRCT. Although radiological abnormalities have prognostic relevance in patients with extensive involvement [5,17], in the Diamond Princess Ship study, half of the asymptomatic patients had pathologic findings on HRCT [18]. suggesting a limited specificity of this technique. Thus, HRCT extension alone may not be a good predictor of worse outcomes in patients presenting to the ED without respiratory failure. In this context, we used a lung ultrasound, which is a safe and reproducible tool for the longitudinal evaluation of the severity of pneumonia, as previously described [19].
The previously reported experiences of the outpatient management of the pandemic differ from our study in substantial ways [8,9]. For example, Teigell Munoz et al. [8] screened COVID-19 patients in the ED for minor and major prognostic risk factors, proposing a management strategy with remote follow-up using a questionnaire for clinical status, and patients were sent back to the ED as needed. They enrolled 314 patients and found that of the 19.7% of the patients that were revaluated in the ED and the 6.4% that were hospitalized, none died. Conversely, Llorens et al. [9] described findings from 109 patients that were discharged from the ED, revaluated after 24 hours, and then cared for by home nursing visits. In this study, 19.2% of the patients were sent back to the ED (the primary outcome), and 6.2% were hospitalized.
The population of our study was at a higher risk of progression than the two previously reported Spanish cohorts [8,9]. That is, our patients had a mean age of 63 years (versus 45 and 50), all with one or more comorbidities (versus 42.2% and 19.9%), a mean PaO2/FiO2 ratio of 357.5 (versus 488 and not reported), and all had documented HRCT+ pneumonia (not reported in either of the previous studies). Second, during the follow-up period, patients were revaluated directly in the ED, performing a more reproducible assessment, while in the other studies the follow-up strategy was a phone call questionnaire or a nursing visit, which may be useful for low-risk patients, but probably not feasible for our cohort.
A notable strength of all the home protocols was the possibility of measuring patients’ oxygen saturation at home and performing a QWT. More recently, several other studies reported the favorable experience of using telemedicine or remote monitoring in COVID-19 patients, all of which included the home measurement of oxygen saturation with a pulse oximeter [20-22]. For example, in a study by Gootenberg et al. [20] approximately 10% of the patients that were initially discharged from the ED were admitted late to the hospital, as were 7% of them in the study by Tabacof et al. [22] which is a slightly lower rate than in our cohort (17%).
During a pandemic, the optimization of resources is crucial. Although we were able to provide only an indirect comparison with a cohort of comparable patients, adopting a “discharge and early revaluation” strategy may have spared many hundreds of hospitalization days, considering that without the ambulatory management most, if not all, of the enrolled patients would have been hospitalized. This is also important because, to date, no therapies have been demonstrated to be effective for SARS-CoV-2-related pneumonia in patients without respiratory failure [23].
The study has several limitations. First, this study was conducted in a single center with a small cohort of patients, so the data may not be generalizable, especially regarding organizational aspects and regional management (our hospital was a hub center for COVID-19). The inclusion criteria were established with a multiparametric evaluation that may have introduced selection and information bias. Furthermore, there were no absolute indications for the hospitalization in the control visit as it was left to the judgment of the medical staff. The control group was selected from a historical cohort to match low-risk patients that were managed as inpatient, but this determined a selection of patients and an incomplete matching of data.
In conclusion, our study demonstrates that COVID-19 patients without respiratory failure can be safely managed with a “discharge and early revaluation” approach directly from the ED staff. This translates into similar outcomes for the patients but with a significant saving of resources for the national health system. Further studies are needed to assess the best management strategy for low-to-moderate risk COVID-19 patients.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We thank Maria Capalbo for her authorization and support.
References
Article information Continued
Notes
Capsule Summary
What is already known
Many different outpatient strategies were adopted during the severe acute respiratory syndrome coronavirus 2 pandemic, but they included patients without pneumonia or with mild disease.
What is new in the current study
The strategy described should be helpful in the management of COVID-19 patients with mild-to-moderate pneumonia as outpatients, sparing resources without losing in safety.