INTRODUCTION
Dyspnea is an abnormally uncomfortable awareness of breathing [1]. In 2014, dyspnea was the cause of 3.4 million emergency department (ED) admissions and accounted for 2.4% of total ED visits in the United States [2]. In patients aged older than 65 years, dyspnea is the third most common cause for ED admissions in the United States. Acute dyspnea is associated with many pathologies and is thus a challenge for the emergency physician. Differentiating between its causes may be difficult, particularly in elderly patients with multiple comorbidities. The most common pathologic causes of dyspnea include heart failure, chronic obstructive pulmonary disease (COPD), and pneumonia. However, there are several other causes of dyspnea that can be fatal, and these may require special diagnostic modalities that are potentially complicated, expensive, and invasive. Moreover, other pathologies of dyspnea require high-risk treatment regimens.
A rapid and accurate diagnosis is tantamount to early determination of appropriate intervention. Numerous studies have demonstrated an increased short-term mortality risk when appropriate interventions are delayed, which may occur when diagnosis is deferred [3-5]. Further, large studies have shown increased mortality when treatment is delayed as this also results in prolonged ED stay [6,7]. However, there is no single historical, physical examination, electrocardiographic (ECG) or radiographic finding that can accurately and independently diagnose the pathologic cause in patients presenting with dyspnea [8].
Because ultrasound allows for rapid, inexpensive, and non-invasive assessment of many different organs, it may be valuable in ED patients with acute dyspnea [9]. Further, it may have unique diagnostic characteristics that cannot be obtained by other standard ED investigations in patients presenting with acute dyspnea. Ultrasound can be used to evaluate the potential for interstitial lung fluid as it can detect B-lines, which have a high diagnostic accuracy for distinguishing acute dyspnea of cardiac etiology from that related to pulmonary diseases (e.g., COPD) [10]. Although B-lines are not specific for cardiogenic pulmonary edema and can be seen in other respiratory disorders such as acute lung injury and acute respiratory distress syndrome [11], their presence combined with other parameters, i.e., left ventricular (LV) systolic function [12] and collapsibility of inferior vena cava (IVC), may help identify abnormal volume states (e.g., sepsis, dehydration, hemorrhage, or heart failure) [13].
However, few studies have evaluated the diagnostic accuracy and temporal impact of ED ultrasound in a randomized blinded manner in patients presenting with acute dyspnea. This study aimed to determine the diagnostic accuracy and temporal impact of ultrasound in patients with acute dyspnea admitted to the ED compared with standard therapy. Moreover, we also aimed to determine and compare the time required to obtain an accurate diagnosis in patients randomized to a standardized ultrasound strategy and standard care.
METHODS
Trial design
This was a parallel, block randomized, standard therapy controlled, blinded evaluation of a point-of-care ultrasound strategy in adult ED patients presenting with a chief complaint of shortness of breath. The trial was approved by the institutional ethics committee (H-38431) and used a convenience sampling method (when the ultrasonographers were available) for patient enrollment. The patient’s allocation ratio was 1:1, and no changes to the methods were made after the start of the trial.
Participants
This study was conducted at a large urban public hospital ED with an annual census of >100,000. We enrolled patients from March 2016 to April 2017. All patients were followed up during their ED stay. The medical records were reviewed 30 days after the index visit to determine the final diagnosis.
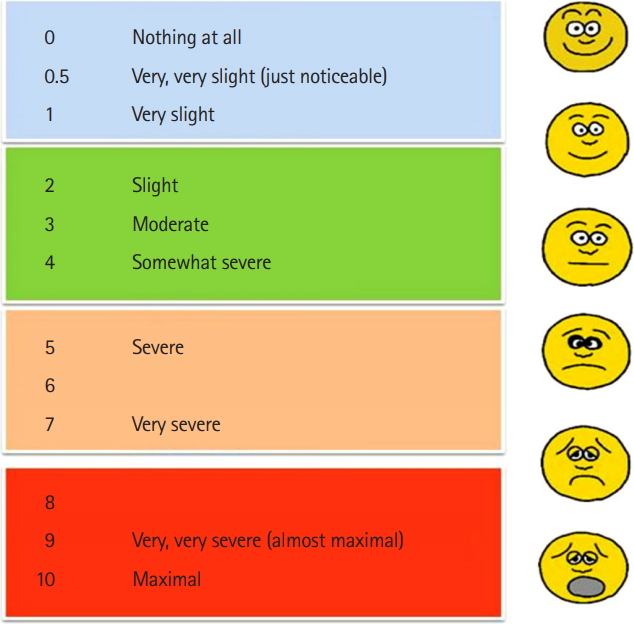
Patients were enrolled if they met the following inclusion criteria: age >18 years and shortness of breath of at least moderate severity as determined according to the modified Borg dyspnea scale [14] and a 100-point visual analogue scale (VAS) (Figs. 1, 2). Patients were excluded if they had ECG changes consistent with ST segment elevation indicative of myocardial infarction, a Modified Borg Scale >8, or the treating physician had already received the results of non-ECG diagnostic test (i.e., lab or chest radiography findings), thereby disrupting blinding.
Trial intervention
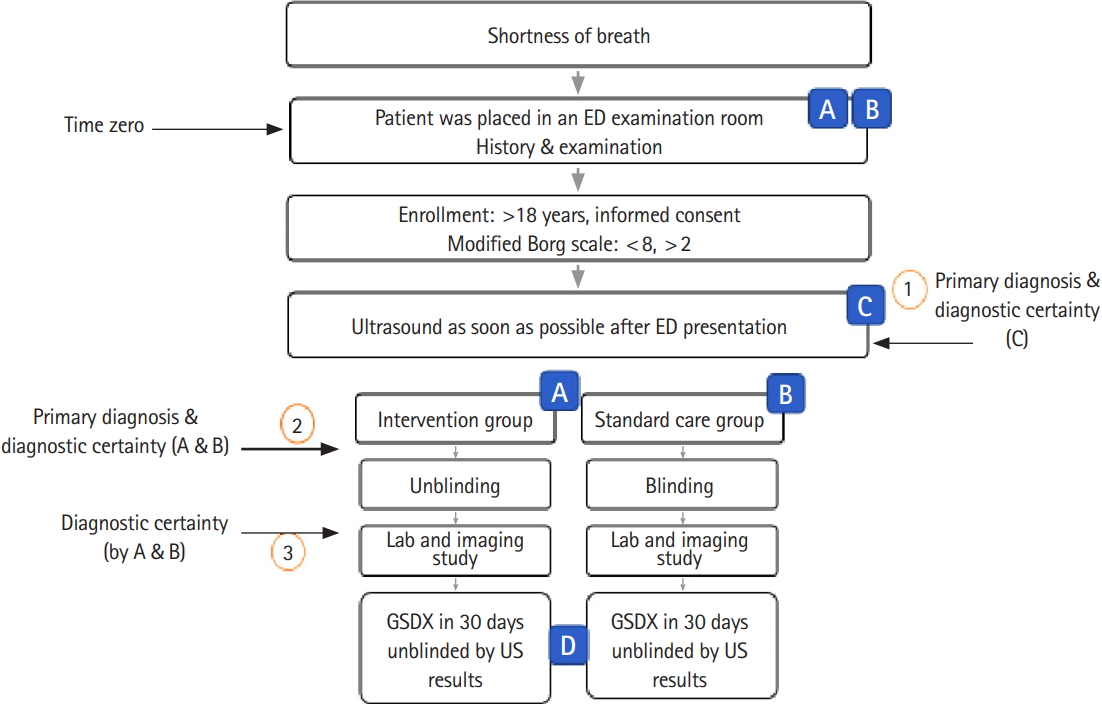
Blinded ultrasounds were performed as soon as possible after ED arrival once informed consent was obtained. The patients were then randomized according to whether their treating team was unblinded (group A) or not (group B) to their ultrasound results. All patients received standard care. The study flow is presented in Fig. 3. Time zero was defined as the time the patient was placed in an ED examination room.
Ultrasound scanning was performed by trained ED physicians. Scanners were blinded to the patient’s medical history and were not allowed to be involved in any diagnostic or therapeutic patient care discussions.
In the unblinded ultrasound cohort (group A), before unblinding the ultrasound results, the primary physician was asked to document their primary diagnosis and their diagnostic certainty using a 10-cm VAS (Fig. 4). Ultrasonographers were also asked to provide a primary diagnosis and diagnostic certainty (group C) (Fig. 3). To evaluate diagnostic change as a function of ultrasound results, diagnostic certainty was reported a second time by the primary physician 10 minutes after receiving the ultrasound results, in the unblinded cohort (Fig. 4).
Standardized ultrasound procedure
Ultrasound scanning was performed by one of four emergency medicine physicians, each with at least 2 years of practice experience, and all of whom had completed an ultrasound fellowship. All patients were evaluated using a phased array probe, with a range of 1 to 3 MHz (Edge; SonoSite, Bothell, WA, USA). The required standardized ultrasound approach included echocardiography, an IVC evaluation, and a lung exam.
Cardiac ultrasound was performed with visual assessment of the global LV systolic function from as many views as possible. The ratio between the right and left ventricles was visually assessed and then recorded. Pericardial effusions, LV hypertrophy, or any other observed cardiac pathology were also recorded.
Bilateral scanning of the anterior, lateral, and posterior chest walls was performed with the patient in the supine or sitting position (Fig. 5) [15]. The chest wall was divided into three zones: anterior (from the parasternal line to anterior axillary line), lateral (from the anterior axillary line to the posterior axillary line), and posterior (posterior axillary line to the paravertebral line). Each zone was then further divided into upper and lower areas. This resulted in a total of 12 areas scanned for each patient. The investigator recorded the presence of A and B lines, pleural effusions, hepatization, air bronchogram, or any other noted lung pathology.
The IVC was evaluated within 2.0 cm of the IVC-right atrium junction. The IVC diameter was expressed as no respiratory variation, minimum respiratory variation (<50% collapse of the IVC diameter), or significant respiratory variation (>50% collapse of the IVC diameter). Ultrasound diagnoses were ultimately defined according to the following criteria [16]:
Heart failure with preserved ejection fraction (HFrEF) with pulmonary edema: Lung scan would show diffuse interstitial pattern (or diffuse B-pattern, >3 B-lines in a rib space in at least 2 among 4 anterolateral areas of each hemithorax bilaterally.
HFrEF with pulmonary edema: Lung scan would show diffuse interstitial pattern (or diffuse B-pattern, >3 B-lines in a rib space in at least 2 among 4 anterolateral areas of each hemithorax. Cardiac scan: reduced EF on visual assessment of the global LV systolic function. IVC scan would show minimum respiratory variation during inspiration (<50%).
Airway diseases diagnosis is made by exclusion, if nothing was found on the ultrasound scan, AND includes asthma and chronic obstructive pulmonary disease.
Pneumonia is diagnosed by absence of lung sliding with B-lines, consolidation, OR focal interstitial pattern.
Pleural effusion is diagnosed by the presence of anechoic or black fluid collection between the visceral and parietal pleura in a dependent pattern.
Pericardial effusion is diagnosed by the presence of anechoic or black fluid collection in the pericardial cavity, usually best visualized in the subcostal view.
Pneumothorax is diagnosed by absence of lung sliding, the presence of a “lung point” or a “transition point” (defined as the presence of normal lung sliding and no lung sliding at the pneumothorax border).
Gold standard diagnosis
The gold standard diagnosis was determined by two independent emergency physician reviewers who were not involved in the study or patient care and blinded to all ultrasound results and to each physician’s diagnosis. They reviewed all available clinical data at least 30 days after the index ED visit. The final gold standard diagnosis was defined as both reviewers having the same diagnosis. In cases where the reviewers had different diagnoses that persisted after discussion, a third physician, blinded to all study ultrasound data, resolved the disagreement.
Statistical analysis
As this was an observational study, no pre-specified power analysis was performed. Patients were randomized using a 4-subject block randomization scheme. The ultrasonographer determined the group allocation by opening a single sequentially numbered opaque envelope containing the randomization result. In 50% of the patients, the treating physician was aware of the ultrasound results, while in the other 50%, the ultrasound results remained blinded. Data were analyzed with descriptive statistics using Stata ver. 14 (StataCorp., College Station, TX, USA). The sensitivity, specificity, accuracy, positive predictive value, and negative predictive value of the standardized ultrasound strategy for an accurate gold standard diagnosis of dyspnea is presented. Statistical analyses were performed with z-test. Times of diagnosis, treatment, and disposition decision were presented as mean±standard deviation, and Student t test and chi-square test was used for continuous and categorical data analysis.
RESULTS
Patient characteristics
Of the 60 patients enrolled, one left against medical advice before the final diagnosis was made. Thus, 59 patients were randomized to the standard of care cohort (ultrasound data remained blinded, n=30) and unblinded ultrasound cohort (n=29). The mean±standard deviation age was 54.4±11 years, and 37 (62%) were male. Racial distribution was 31 (51.5%) African Americans, 24 (40%) White, 2 (3.4%) Asians, 2 (3.4%) Indians, and 1.7% other races. Patients were enrolled by 12 emergency physician faculty and 16 residents with different levels of experience. The patients’ demographic data are presented in Table 1. There were no significant differences between the blinded ultrasound control and the unblinded ultrasound cohorts. The median (interquartile range, IQR) time from ED arrival to bed placement was 23.5 (7.25 to 47.5) minutes, with randomization occurring at 79 (49 to 122) minutes. The 55.5-minute time from bed placement to randomization was a consequence of obtaining informed consent.
Diagnoses
The median (IQR) time from randomization to ED diagnosis was 21 (10 to 15) minutes for unblinded ultrasound patients versus 244 (128 to 360) minutes for standard of care blinded ultrasound group (P<0.001) (Table 2). The final adjudicated diagnoses and ED disposition are listed in Table 3. Overall, HFrEF and “other” diagnoses accounted for almost 50% of diagnoses in the enrolled patients (23.8% for each), followed by airway diseases (asthma/COPD), non-specific chest pain, and pneumonia. Patients had high rates of severe illness, as reflected by high rates of intensive care unit admission. A total of 60% of patients with pneumonia, 36% of patients with heart failure, and nearly 20% of patients with airway diseases were admitted to the intensive care unit, respectively.
Diagnostic accuracy
Diagnostic accuracy in both unblinded and blinded ultrasound physician with access to clinical information (groups A and B, respectively) was 76% (Table 4). This was similar to the diagnostic accuracy (79%) of group C (the ultrasonographers without clinical information) (P>0.796). When stratified by diagnosis, accuracy was similar across all groups, and was similar for the specific diagnoses of heart failure and airway disease. While both the unblinded and blinded ultrasound groups had similar diagnostic performance for HFrEF, both missed 2 cases. Finally, while the unblinded standardized ultrasound strategy had a higher sensitivity than standard care for pneumonia, it had lower specificity and positive predictive value.
Diagnostic certainty is crucial to a physician’s ability to initiate treatment. Unblinding of the ultrasound results had minimal effect on diagnostic certainty, planned therapy, or disposition decision. In the standardized ultrasound strategy cohort, initial diagnostic certainty was 73% (95% confidence interval [CI], 65% to 82%) and increased to 78% (95% CI, 67% to 87%) (P=0.559) after un-blinding. Only 8 physicians changed their level of certainty; 7 became more confident and 1 became less certain of their diagnosis. Additionally, unblinding of ultrasound results did not change the planned disposition; only 1 physician changed their disposition with unblinding (from home to admission). Finally, although group A was unblinded to the ultrasound results, no physician changed their management plan. They preferred to use the standard of care to reach the diagnoses; therefore, there were no significant differences between group A and group B regarding time to diagnosis or ED length of stay. Overall, no harms or unintended effects occurred in any subgroup.
Despite being blinded to the patients’ history and physical exam findings, ultrasonographers were asked to document their diagnoses. Evaluation of the entire sample found that the ultrasonographers (group C) had higher diagnostic certainty after scan completion than the treatment team (groups A and B) before the ultrasound results were known (82% [95% CI, 77 to 87] vs. 74% [95% CI, 69% to 79%], P=0.018).
Overall, the median (IQR) ED length of stay was 8.0 (6 to 11) hours, during which dyspnea severity was evaluated hourly with the VAS and modified Borg scale. In general, dyspnea severity improved during the patient’s ED stay. The median (IQR) VAS severity of dyspnea at the time of enrollment was 75 (50 to 80), improving to 50 (40 to 60) over 4 hours (P<0.001).
DISCUSSION
In this study, the use of a standardized ultrasound strategy resulted in more rapid, but equally accurate diagnoses, as compared to standard of care in ED patients presenting with acute dyspnea. This finding has operational implications in busy EDs and may allow potential outcome improvements in patients with high severity of illness where diagnostic delays may be associated with worse outcomes. The time to obtain a correct ED diagnosis is important. In a study of 14,900 heart failure patients admitted to the ED [3], delayed furosemide administration was associated with increased mortality. In another study of 35,000 heart failure patients admitted to the ED [4], delayed vasoactive treatment was associated with increased rates of acute death. Our findings that ultrasound allows for a more rapid HFrEF diagnosis in ED patients presenting with dyspnea indicates that our standardized ED ultrasound strategy could improve HFrEF outcomes.
Our study has a number of unique features, the most important of which is that we investigated the diagnostic accuracy and operational efficiency of ultrasound and its impact in the ED through a single evaluation. First, we validated the accuracy of our standardized ultrasound strategy versus standard care and demonstrated equal performance between the two. Second, as the physicians performing the ultrasound were blinded to the patients’ history and physical exam findings, we could determine the independent contribution of performing the ultrasound to diagnostic certainty. Third, by timing the interval to diagnostic results, we quantified the time saved from the standardized ultrasound strategy as compared to that in standard care. Unlike other studies [16-19] that evaluated various parts of our approach, our finding of a 4.5-hour earlier time to accurate result is likely to have important operational and clinical outcome relevance in the ED.
Others have reported subsets of our study. Gallard et al. [17] demonstrated a mean±standard deviation time to complete a cardiopulmonary ultrasound of 12±3 minutes, which was similar to our median (IQR) time of 12 (3 to 18) minutes. However, they did not perform an IVC exam and did not include data regarding time for standard of care diagnosis. Another study by Zanobetti et al. [18] used ultrasound and standard care reporting similar to our investigation, e.g., lung, cardiac, and IVC ultrasound, but without blinding. They reported similar mean±standard deviation times of 24± 10 and 186±72 minutes for ultrasound and standard of care diagnostic time, respectively. Finally, both Mantuani et al. [19] and Papanagnou et al. [20] found that the most common final diagnoses in patients presenting to the ED with acute dyspnea were heart failure, airway disease, and pneumonia, which is similar to our findings.
In our analysis, the overall diagnostic accuracy of the standardized ultrasound strategy was similar to standard care (76% vs. 78%, P=0.796). Meanwhile, other studies have reported diagnostic superiority for this type of strategy. The SEARCH8Es protocol reported an accuracy of 90.1% and superiority over standard care (P<0.001) [21]. Importantly, their ultrasonographers were not blinded to patient data, the points of their scans varied based on their differential diagnosis, and their post-scan diagnosis was chosen from a list limited to 13 options.
Compared with standard care, our standardized ultrasound approach was more sensitive (83 vs. 66%) for diagnosing pneumonia, but it had lower specificity (75.9 vs. 98.1). Others have reported similar results. In a meta-analysis of 1,551 patients, Long et al. [22] reported an ultrasound sensitivity of 88% (95% CI, 0.86 to 0.90), with a higher specificity (86%; 95% CI, 0.83 to 0.88) than our analysis. This may be because we did not define sonographic criteria for pneumonia, which allowed for more diagnostic variation.
Finally, our study found a high sensitivity of 90.9% (95% CI, 83.5% to 98%) for diagnosing airway disease, which was similar to standard care. Prior studies have shown lower sensitivities. The SEARCH8Es reported the sensitivity of ultrasound to be as low as 76.5% in patients with airway disease and sepsis [21]. The reasons for their less than expected performance may be explained by their relatively small number of patients with airway disease or sepsis (n=30) and that airway diseases, such as asthma or COPD, may require more extensive lung evaluations than those that were mandated by their protocol. In our study, there were four false-positive cases of posterolateral alveolar/pleural syndrome in patients with COPD; these patients were ultimately found to have no pneumonia. This finding was comparable to that of SEARCH8Es, in which three patients with airway disease were identified to have normal lung patterns but subsequently found to have abnormal pulmonary functions after admission.
We found that our standardized ultrasound strategy did not significantly change the physician’s diagnosis, although we observed a modest increase in their diagnostic confidence. This finding is in contrast to that of Papanagnou et al. [20] who reported a moderate increase in diagnostic confidence and some changes in management. Consistent with the lack of a change in diagnosis, we found that un-blinding the ultrasound data did not change therapy or disposition decisions. This may be a function of a lack of confidence in the ultrasonographic findings as reported to the treating team with unblinding. Interestingly, ultrasonographers demonstrated considerably higher levels of diagnostic certainty despite being blinded to the clinical scenario.
Our study has several limitations. These include its small sample size and single-center enrollment that may have restricted some of our findings. Our study did not include patients with severe dyspnea (defined as a Borg dyspnea score >8) as this group is unable to provide informed consent. This may limit the generalizability of our results to the population studied. However, our findings can be a basis for future studies to include a more severely dyspneic cohort. We also enlisted only fellowship trained ultrasonographers, whose skill sets may not be duplicated elsewhere. Additionally, our convenience sampling design, with enrollment occurring when the investigator and the ultrasonographers were in the ED simultaneously, may have resulted in unmeasured bias. Finally, there was no pre-specified agreement on the pneumonia diagnostic criteria, which may have decreased the sensitivity of the ultrasound data.
In conclusion, compared to standard of care, a standardized ultrasound strategy is diagnostically as accurate, but provides much earlier diagnosis, saving more than 4.3 hours in the evaluation of patients presenting to the ED with acute dyspnea.