INTRODUCTION
Optimum chest compression is critical for successful cardiopulmonary resuscitation (CPR). The current CPR guidelines have emphasized a specific rate (100ŌĆō120 beats/min), depth (5ŌĆō6 cm), full recoil after each compression, and minimizing pauses for compression [1,2]. However, they allow a relatively broad range region, the lower sternal half (approximately 9 cm), to compress [3].
This compression site for the general population has been determined by the studies that assumed that the stroke volume (SV) of the left ventricle (LV), a key point for successful CPR, would be maximized by compressing the theoretical optimum ŌĆśpointŌĆÖ (P_max.LV) beneath which the LV is at its maximum diameter [3-11]. Using these rationale, the authors suggested that ŌĆśpersonalized P_max.LVŌĆÖ should be compressed considering the wide variations in cardiac locations among individuals. Additionally, it was suggested that it would be important to determine ŌĆśpersonalized P_max.LVŌĆÖ using posteroanterior chest radiography (chest_PA), as patients suffering from myocardial infarction are considered for personalized therapy [12-14]. Assuming that the relative location of P_max.LV within the heart would be constant universally, we mathematically derived and validated rules to locate P_max.LV using simple parameters measured on chest_PA, including cardiac diameter, right cardiac border, and cardiac height (Fig. 1A) [12].
To apply the rules without the interruption of CPR, chest_PA should be performed before the cardiac arrest (CA). Due to the lack of previously investigated chest_PAs, these rules are applicable to only 71% and 38% of in-hospital CA (IHCA) and out-of-hospital CA (OHCA) victims, respectively [12]. This limited applicability might have reached up to 100% and 60%, respectively, if P_max.LV had been estimated using anteroposterior chest radiography (chest_AP). Chest_PA requires patients to stand up alone and take a deep breath; critically ill patients who are unable to do this are required to undergo portable chest_AP instead. As such patients at a higher risk for CA, need more urgent and proactive determination of personalized P_max.LV [15-17].
In this study, we aimed to derive and validate the rules to determine personalized P_max.LV using the chest AP. We used the same methods as Cho et al. [12] except we used chest_AP instead of chest_PA. First, we identified the 3D coordinates of P_max.LV on computed tomography (CT) which is the reference standard test. Subsequently, we derived and validated rules to estimate each coordinate using parameters which were easily measurable on chest_AP.
METHODS
Design, setting, and participants
In this retrospective cross-sectional study, we included all consecutive non-CA adults aged Ōēź18 years who had undergone chest_AP within 1 hour of CT with sagittal reconstruction from 2012 to 2017 in CHA Bundang Medical Center. The institutional review board of the hospital approved this study protocol (2018-06-016-002). The requirement for informed consent was waived for this retrospective study.
We excluded cases that required alteration in cardiopulmonary modifying medications between performing chest_AP and CT (anti-hypertensives, diuretics, inotropics, chronotropics, fluid loading, beta agonists, and anticholinergics) and those with any immeasurable parameters on either test. Cases with the following thoracic abnormalities were included as they were found not to affect the rules in the determination of P_max.LV in the previous study: >2-cm depth pleural effusion, >1-cm depth hemo-/pneumothorax, a destroyed lung, lobectomy, atelectasis, hiatal hernia, >5-mm depth pericardial effusion, pericardial tumor/cyst, thoracic aorta dissection/aneurysm, and widened mediastinum [12]. We assigned enrolled cases randomly to derivation and validation sets using a 3:2 ratio, respectively.
Definition of structures on chest_AP, the chest surface, and CT
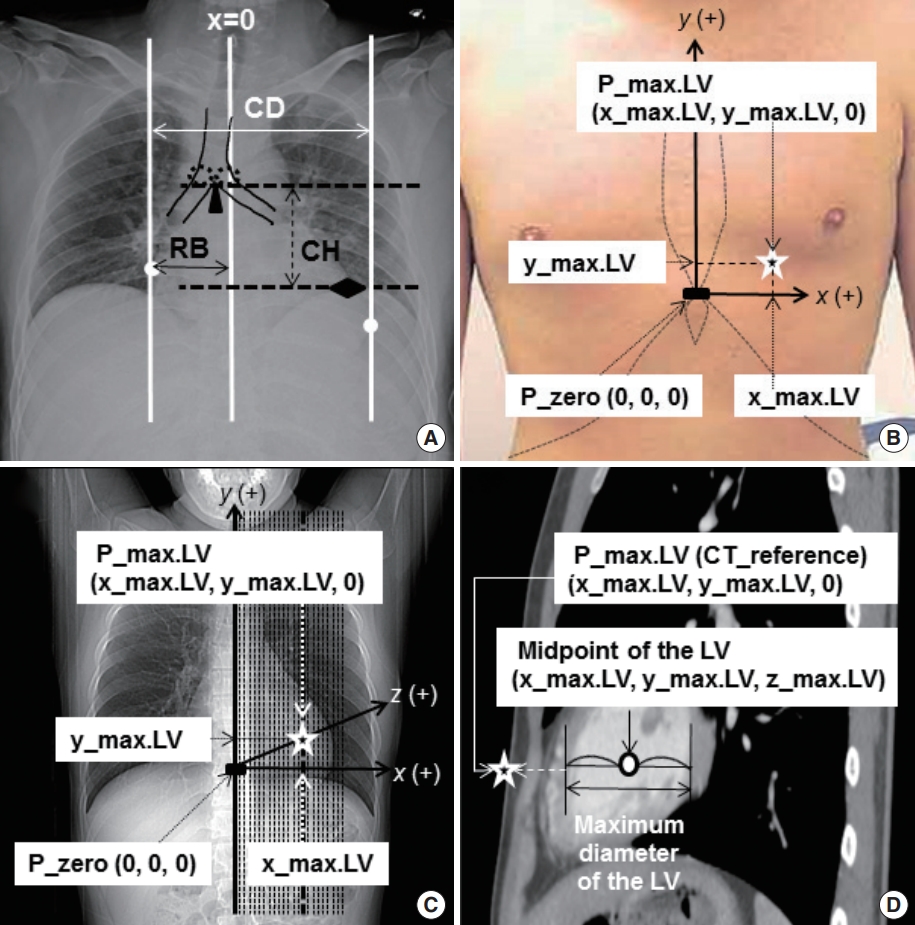
We defined anatomical structures on chest_AP, the chest surface, and CT as described by Cho et al. [12] From the chest_AP, cardiac diameter (CD) was defined as the distance from the right cardiac border (RB) to the left one. We defined cardiac height (CH) as the distance from the bottom of the carina to the uppermost point of the left hemi-diaphragm (Fig. 1A) [12].
The reference point, (P_zero [0, 0, 0]), was defined as the midpoint of the xiphisternal joint on both the chest surface and CT. Leftward, cephalad, and into-the-thorax directions were designated as positive on x-, y-, and z-axes, respectively (Fig. 1B, C) [12].
The midpoint of the LV where it showed the maximum diameter was identified using CT as follows: x_max.LV, y_max.LV, z_max.LV. P_max.LV, which was assumed to be located just vertically above that point on the chest surface (z=0), was then positioned at the following location: x_max.LV, y_max.LV, 0 (Fig. 1C, D) [12].
Mathematical derivation of the rule to estimate P_max.LV
Assuming that the relative location of P_max.LV within the heart does not change interpersonally, its proportional width and height compared with CD and CH would remain constant. Using this assumption, we have inferred the following rules to estimate x_max.LV and y_max.LV, where ╬▒0, ╬▓0, and ╬│0 were constants derived from the study population [12];
x_max.LV=╬▒0*CD-RB
y_max.LV=╬▓0*CH+╬│0
(For detailed mathematical inference, please see explanation S1 of reference number 12).
Using the derivation set, we measured x_max.LV and y_max.LV on CT; and CD, RB, and CH on chest_AP. Using these measurements, we defined ╬▒0 as the mean value of ŌĆś(x_max.LV+RB)/CDŌĆÖ. ╬▓0 and ╬│0 were determined as the representative regression coefficient and constant, respectively, revealed on the linear regression analysis to express y_max.LV in terms of CH. We then investigated whether the assumptions of the linear regression analysis were met. By determining ╬▒0, ╬▓0, and ╬│0 mentioned as above, we could derive the rules to estimate x_max.LV and y_max.LV to locate P_max.LV.
Validation of the rule to estimate P_max.LV
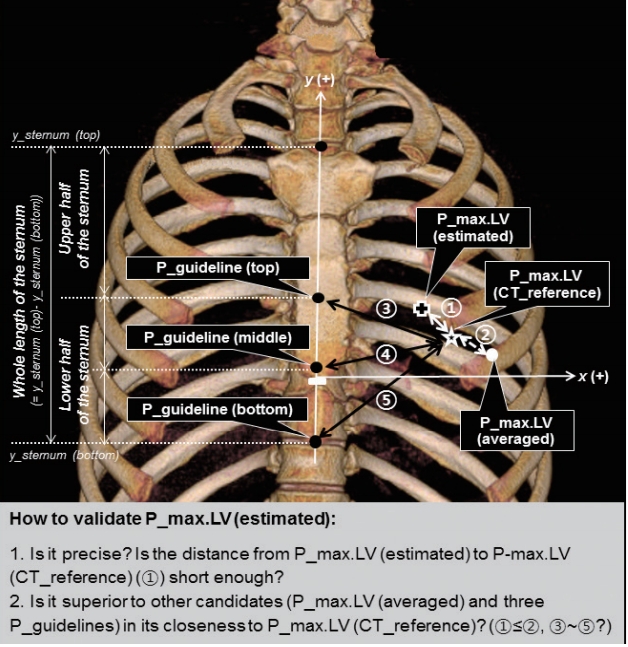
We validated the derived rules to estimate P_max.LV in two ways (Fig. 2). First, to assess the precision of the estimated P_max.LV (P_max.LV [estimated]), we compared its coordinates with those of the reference point identified using CT (P_max.LV [CT_reference]).
Second, we checked the superiority of P_max.LV (estimated) over two kinds of candidate compression points. Thus, we compared the proximity of P_max.LV (CT_reference) to P_max.LV (estimated) with that of each candidate point. The first candidate was P_max.LV (averaged). We defined its coordinates as the mean value of x_max.LV and y_max.LV of all enrolled cases. The second candidate was three P_guidelines to represent the compression site recommended in the current CPR guidelines [1,2]. These were located along the lower mid-sternal half at the same interval from the top to the bottom per individual as P_guideline (top), P_guideline (middle), and P_guideline (bottom).
Comparison with the previous study to determine P_max.LV with Chest_PA
In order to compare the results of the current study with those from the previous study in which we determined P_max.LV using chest_PA, we compared the variables using unpaired t-tests, chi-square tests, and others [18].
Measurement of variables
One author (KS) measured all parameters in all patients. To verify interrater reliability, another (CS) measured CD, RB, CH; x_max.LV, y_max.LV, and y coordinates of the sternal top (y_sternum [top]) and bottom (y_sternum [bottom]) among 8% of cases that were randomly selected. The intra-class correlation coefficient was calculated for each variable.
Data on sex, age, height, weight, and comorbidities were obtained from patient medical records. Body mass index was calculated as ŌĆśweight (kg)/height (m)2ŌĆÖ.
Statistical analysis
Demographic information, comorbidities, parameters on chest_AP and CT, and ╬▒0, ╬▓0 and ╬│0 were shown in derivation, validation, and combined sets. Continuous variables were presented as mean┬▒ standard deviations and were compared using t-tests. Categorical variables were presented as proportions (%) and were compared using chi-squared tests.
We defined type 1 and 2 errors as <0.05 and <0.10, respectively. Expecting the correlation coefficient (r) to be >0.25 for the linear regression analysis to estimate the y_max.LV with CH, the sample size of the derivation set had to be Ōēź164. Allotting cases to derivation and validation sets in a 3:2 ratio and assuming a loss rate as 0.4, we reviewed Ōēź456 cases [19].
Statistical analyses were performed using IBM SPSS Statistics ver. 24 (IBM Corp., Armonk, NY, USA). Statistical significance was presumed when two-sided P-values were <0.05.
RESULTS
In total, 482 patients had chest_AP and CT performed within 1 hour of each other. Among them, 122 cases were excluded: 43 cases for receiving medication between chest_AP and CT and 79 cases for unmeasurable variables in either test. Finally, 360 cases (mean age┬▒standard deviation 52.0┬▒18.3 years, 102 [28.3%] females) were enrolled.
We randomly assigned 237 (65.8%) and 123 (34.2%) cases to the derivation and the validation sets, respectively. There were no significant differences in sex, age, body habitus, comorbidities, and structural abnormalities between the sets (Tables 1, 2).
Intra-class correlation coefficients to reveal the interrater reliability in measuring CD, RB, CH, x_max.LV, y_max.LV, y_sternum (top), and y_sternum (bottom) were all >0.95 (P<0.001, n=30) (Table 3).
With the derivation set, ╬▒0 was 0.643┬▒0.073, showing a normal distribution (Kolmogorov-Smirnov, P=0.20). As the mean of x_max.LV and y_max.LV was 52 and 11 mm, respectively, we located the P_max.LV (averaged) at (52 mm, 11 mm). The assumptions of the linear regression analysis were met to express y_max.LV in terms of CH. The regression analysis revealed the following:
y_max.LV=60-0.425*CH
(r=0.351, ╬▓0: -0.425 [95% confidence interval, -0.556 to -0.294], P<0.001; ╬│0: 60 [95% confidence interval, 45 to 75], P<0.001)
Using those representative statistics, we could estimate P_max.LV as follows:
x_max.LV=0.643*CD-RB (mm)
y_max.LV=60ŌĆō0.425*CH (mm)
We validated these rules by applying them to the validation set (Table 1 and Fig. 2) [12]. The distance from P_max.LV (estimated) to P_max.LV (CT_reference) was 20┬▒11 mm; this did not significantly differ when compared with the distance from P_max.LV (averaged) (19┬▒11 mm) to P_max.LV (CT_reference) (P=0.13). When compared with the distance from the three P_guidelines to P_max.LV (CT_reference), 67┬▒13, 56┬▒11, and 76┬▒18 mm, respectively, it was significantly shorter (P<0.001).
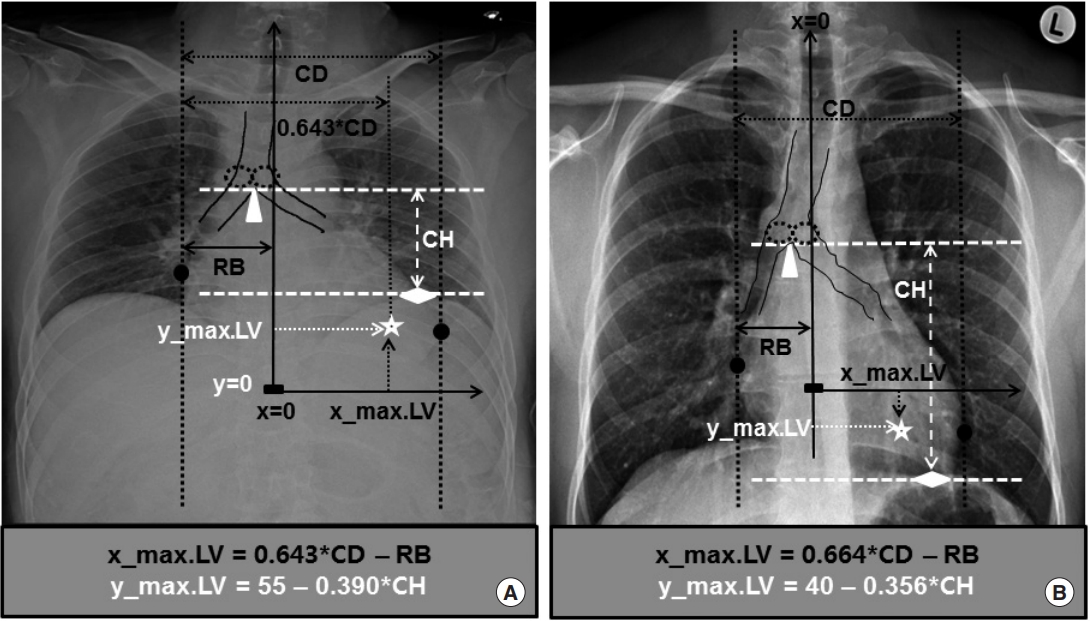
Reanalyzing using the whole set of combined cases, we obtained the following modified rules to estimate P_max.LV on chest_AP (Fig. 3A) [12]:
x_max.LV=0.643*CD-RB (mm)
y_max.LV=55ŌĆō0.390*CH (mm)
When these rules were applied to the whole set, the result of validation was similar (Table 1).
Compared with the previous study that had estimated P_max.LV using chest_PA, the population for whom chest_AP was performed in the current study had fewer women and younger, taller, and heavier individuals (Table 4). Additionally, the population had a larger CD and RB, and a smaller CH, higher y_max.LV, and smaller ╬▒. On linear regression analysis to express y_max.LV in terms of CH, the constant (y-intercept) ╬│ was larger although the slope of ╬▓ did not significantly differ.
The difference between the estimated and reference x_max.LV and y_max.LV did not significantly differ from that of the previous study. However, all the distances from P_max.LV (CT_reference) to P_max.LV (estimated), P_max.LV (averaged), and P_guidelines were larger than those revealed in the previous study based on chest_PA, with the exception of P_guideline (top).
DISCUSSION
This study revealed that the theoretical P_max.LV could be located with parameters easily measurable on chest_AP. We derived and validated its estimating rule as follows: x_max.LV=0.643*CD-RB and y_max.LV=55ŌĆō0.390*CH (mm). For P_max.LV (CT_reference), this P_max.LV (estimated) was as close as P_max.LV (averaged) and closer than any of the three P_guidelines.
To our knowledge, this is the first study to estimate the theoretical P_max.LV using parameters measured on chest_AP. If the clinical effectiveness and safety of this estimation rule is verified in actual CPR, this rule in addition to that using chest_PA might help clinicians locate P_max.LV. Additionally, it might assist in guiding personalized optimum chest compression in up to 60% of OHCA and 100% of IHCA patients with easily available radiography which would have been checked using either chest_PA or chest_AP prior to CA.
Due to its similar study design, this study enhances the merits of the one previously conducted [12]. First, if the effectiveness and safety of its application to actual CA victims is verified clinically in further studies, these rules may be incorporated into the electronic health record system and mobile applications to enhance the estimation of P_max.LV in advance to guide CPR. Prenotification to the receiving hospital by ambulance personnel delivering OHCA victims and anticipative identification of the inpatients with high risk for IHCA would facilitate this process [20]. Second, by locating personalized P_max.LV using plain chest radiography, researchers could investigate whether better outcomes (return of spontaneous circulation, survival to discharge, and good neurological outcomes) were associated with the closer compression of the theoretical P_max.LV during CPR. This is supposed to be located just above the point where the LV is at its maximum diameter [3-10]. Third, compared with P_max.LV (averaged), P_max.LV (estimated) did not differ in its closeness to P_max.LV (CT_reference). However, its wide range means better flexibility to reflect the actual P_max.LV (CT_reference) compared with the fixed P_max.LV (averaged), the coordinate of which is (52 mm, 11 mm). Moreover, it showed superiority over the three P_guidelines, which represent the current guidelines. Lastly, as both chest_AP and CT were performed in the supine position, the doubt raised in the previous study because of chest_PA being performed in the standing position may be diminished.
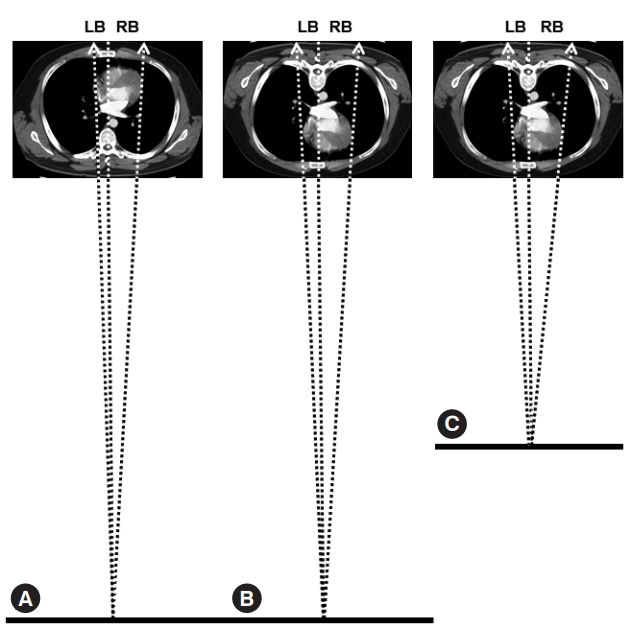
This study showed some differences compared with the previous one, which were not confined to demographic differences that we could not control for (Table 2). First, the population of the study showed smaller CH and higher y_max.LV. When expressing y_max.LV in terms of CH, the constant (y-intercept) ╬│ was larger although the slope of ╬▓ did not differ. This can be explained by the technical differences in chest_PA and chest_AP (Fig. 3) [12]. When taking a chest_PA, the patient is required to stand up and take a full, deep breath. Therefore, the heart, and thus y_max.LV, would be pulled down by gravity and the fully inflated lungs would depress both the heart and diaphragm resulting in a far lower y_max.LV and a larger CH, respectively (Fig. 3B) [12]. Then, the reverse would remain true: a chest_AP would cause a higher y_max.LV and a smaller CH. We were not able to find references to explain the smaller ╬▒ in the current study. We hypothesize that this might be related to the altered heart-lung spatial relationship, such as torsion, which depends on the patientŌĆÖs position and breathing phase, which are the key differences between a chest_PA and a chest_AP. Second, compared with the previous study performed using chest_PA, the population of this study using chest_AP revealed larger CD and RB. This may be explained also by the technical differences in chest_PA and chest_AP (Fig. 4) [21]. In contrast to chest_PA, which is obtained at a fixed distance of 180 cm with the heart located posteriorly, chest_AP is obtained at shorter and variable distances with the heart located anteriorly. Besides the derivation and validation set, we collected a convenience sample of 30 patients to perform a chest_AP in the emergency department. Among these, the mean distance of the radiation was 122┬▒7 cm, ranging from 110 to 132 cm. During chest_ AP, the radiation beam meets the heart at a shorter distance resulting in a larger image of the heart and thus larger CD and RB on the receiving plate for the same patient (Fig. 4) [21].
Initially, we expected that the applicability of the rule to estimate P_max.LV would rise from 71% and 38% to 100% and 60% for IHCA and OHCA, respectively, if P_max.LV became estimable using the previously investigated chest_AP and/or chest_PA. However, we excluded 79 (16.4%) cases among the 482 eligible patients for unmeasurable variables in either chest_AP or CT, thus falling short of that expectation. We think that P_max.LV (averaged) could be used to guide CPR when the estimation rules are not applicable. However, it remains unclear which P_max.LV (averaged) should be adopted; (i.e., the range determined in the previous study [50 mm, -7 mm] or that of the current study [52 mm, 11 mm]).
Comparing the previous study to the current one, x_max.LV was almost the same (50 vs. 52 mm); however, the y_max.LV differed (-7 vs. 10 mm). Both P_max.LVs have been defined on CT, the reference, rather than on chest_PA or chest_AP. Therefore, the difference in y_max.LV would result from the different phase of respiratory cycle during CT rather than the caudal cardiac movement due to the pull of gravity. In the previous study, patients underwent chest_PA; thus, they must have breathed fully during CT. However, those in the current study underwent chest_AP instead of the standard chest_PA, meaning that most of them could not have breathed fully holding their breaths at the end of full inspiration during CT. Their respiratory cycle might have resided even on the expiration phase. The difference in the y_max.LV can be explained by the fact that the LV might move cephalad up to 5 cm at the end of full expiration [22]. However, it remains unclear which estimate of the theoretical optimum chest compression point should be applied; 40ŌĆō0.356*CH (mm) of the previous study measured at the end of full inspiration or 55-0.390*CH (mm) of the current study for those who could not control their breaths.
We think the actual y_max.LV should be determined considering the phase (whether inspiratory or expiratory) of the respiratory cycle during CPR [23,24]. During basic life support (BLS), the successive, uninterrupted 30 compressions after two rescue breaths would shift the lung-to-heart spatial relationship toward the expiratory phase as it lacks in positive-pressure ventilation during chest compression favoring the y_max.LV of the current study. During advanced cardiac life support (ACLS), compression and positive-pressure ventilation via advanced airways are performed asynchronously. As the lung-to-heart spatial relationship will alter throughout the whole respiratory cycle, the y_max.LV might be determined as the one at the mean phase of cardiac movement of the cycle. In a preliminary study performed among 17 CA victims without return of spontaneous circulation despite 30 min of CPR, it was reported that compressing the lowest section of the sternum, thus supporting a lower y_max.LV representing the inspiration phase, might result in a higher peak arterial pressure and end-tidal carbon dioxide [25]. Large-scale clinical studies to enroll CA victims at the scene are needed to clarify the y_max.LV, which if compressed will lead to better clinical outcomes for BLS and ACLS separately, considering the cardiac movement in the respiratory cycle.
This study shares some similar limitations with the one previously conducted [12]. First, CPR was performed throughout the respiratory cycle from the full inspiration by rescue breath to the passive expiration. Some researchers reported that the LV might move cephalad up to 5 cm at the end of full expiration to emphasize the influence of the respiratory phase on the y_max.LV during CPR [22]. However, we cannot control and specify the phase during the entire respiratory cycle when patients undergo chest_AP instead of the standard chest_PA because they usually cannot stand alone or breathe in fully. Regarding the dyssynchrony between chest_AP and CT, we believe it might be limited as we enrolled cases who had these performed within 1 hour of each other. Second, some researchers showed that the LV of pigs in CA moved leftward during BLS and then rightward during ACLS with a maximum deviation <1 cm from the baseline [26]. We could not measure the lateral deviation of P_max.LV in this study as we used static images of the cases without CA.
In conclusion, personalized theoretical P_max.LV, which does not differ from its averaged location and is superior to the locations recommended by current CPR guidelines, may be located with parameters easily measurable on chest_AP. Further clinical studies are needed to verify its effectiveness and safety in addition to modifying its coordinates considering the cardiac movement during CPR by the altering lung-to-heart spatial relationship.