INTRODUCTION
The concept of damage control dates back to World War I with the United States Navy. It is a concept that is used to describe emergency control without definitive repair of a situation that is a threat to a ship and its ability to carry out its mission [1]. The concepts of damage control began to be used in the care of badly injured patients in the 1980’s. Staging care, performing only immediately life-threatening procedures in metabolically deranged patients provided time to correct coagulopathy and complete resuscitation, allowed patients to survive who previously died [1]. The principles of damage control were used originally in patients with penetrating abdominal trauma but now include patients with thoracic and vascular injuries, fractures and other injuries that cause severe physiologic derangements. Damage control involves three phases: control of life-threatening hemorrhage and contamination followed by more complete resuscitation and correction of physiologic derangements, usually in the intensive care unit. The last phase is the definitive management of injuries [1].
PATHOPHYSIOLOGY
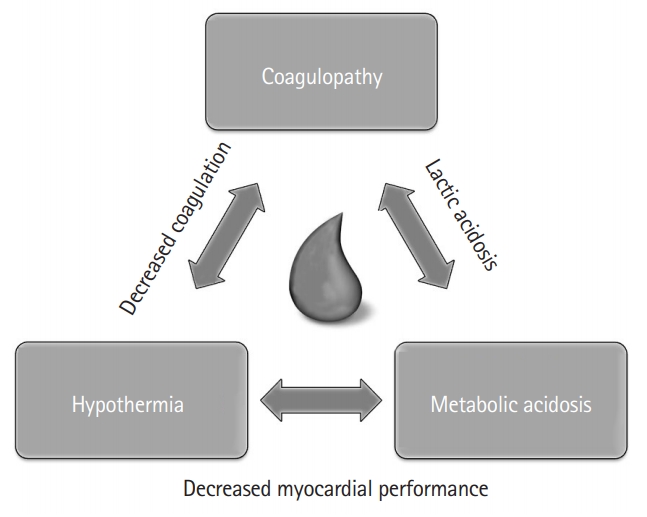
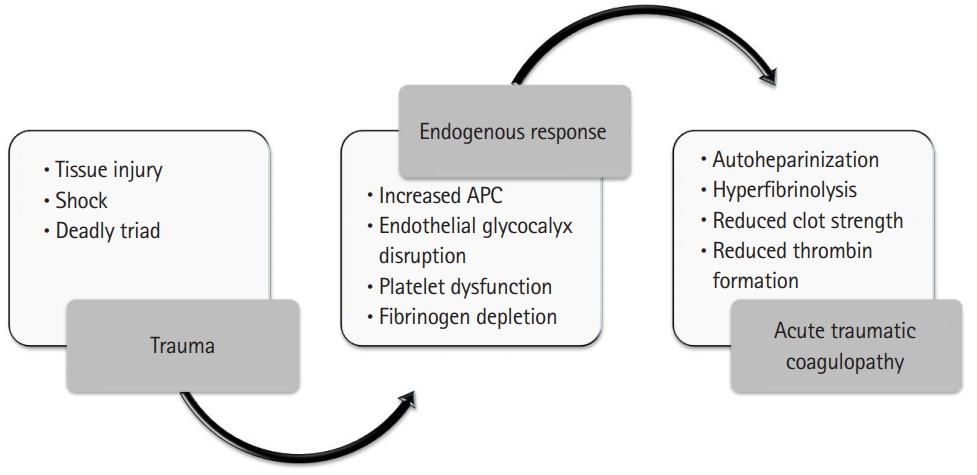
Severely injured patients who sustain large volume blood loss often develop the lethal “triad” of coagulopathy, hypothermia, and metabolic acidosis (Fig. 1) [2]. Each of these disturbances precipitates more of the same, ultimately producing irreversible shock [3]. Significant blood loss, tissue injury and hypoperfusion produces a complex cascade of up-regulated innate immunity genes and down-regulated adaptive immunity genes. Activated protein C, increased plasmin, and a host of other proinflammatory molecules are released, leading to changes in mitochondrial DNA and release of formyl peptides [4]. Acute traumatic coagulopathy manifests clinically as non-mechanical bleeding (Fig. 2) [5,6]. The concept of damage control resuscitation (DCR) recognizes that surgical control of bleeding and resuscitation must happen simultaneously to get the best results. DCR attempts to prevent, rather than treat coagulopathy as the most “treatable” arm of the lethal triad [7,8].
TENETS OF DCR
DCR emphasizes novel resuscitation strategies that attempt to limit secondary blood loss and prevent the development of coagulopathy. These start at the time of patient presentation and continue through the entire phase of resuscitation [8-14]. The principles of DCR are not mutually exclusive of damage control surgery (Fig. 3). Use of this approach has been demonstrated to improve mortality, facilitate earlier abdominal closure, decrease healthcare costs, and decrease length of stay [9,11,15-17]. These include hypotensive resuscitation techniques, early airway control, early use of blood and blood products, and other hemostatic agents.
HYPOTENSIVE RESUSCITATION
Hypotensive resuscitation is an integral part of DCR. Hypotensive resuscitation restricts the use of crystalloid fluids allowing blood pressure to remain lower than normal, limiting secondary blood loss until initial hemostasis can be accomplished. Accepting a lower blood pressure during trauma resuscitation has long been recognized as helpful. Yet, leaving blood pressure low is often counterintuitive to clinicians due to the misconception that blood pressure always equates to organ perfusion [18,19]. During World War I, the Harvard Medical Unit, run by Walter Cannon and John Fraser, observed that when higher blood pressures were targeted with the administration of more crystalloid fluid, “blood that is sorely needed may be lost [20].” In World War II, the same observation was made by Henry Beecher; a systolic blood pressure (SBP) goal of 80 to 90 mmHg was deemed “beneficial” before surgery [21]. A series of animal studies also demonstrated improved survival when lower blood pressures (i.e., mean arterial pressures [MAP] of 50–60 mmHg) were targeted in models of hemorrhagic shock [22]. In most animal models, a MAP of 45 to 50 mmHg was sufficient to maintain brain and heart perfusion and renal perfusion appeared to be maintained when MAP was sustained above 50 mmHg after blood loss [22-24].
The first high-quality human study investigating hypotensive resuscitation was performed by Bickell et al. in 1994 [25]. In this prospective randomized controlled trial that included 598 penetrating torso trauma patients, withholding fluid resuscitation (lactated Ringer’s solution to maintain a SBP >100 mmHg) until arrival in the operating room improved mortality; an 8% mortality benefit was observed including patients with pericardial tamponade [25]. A study by Dutton et al. [26] included both penetrating and blunt trauma patients. Titration of fluids to maintain a SBP >100 mmHg compared to a target SBP of 70 mmHg did not increase mortality in this study of 110 patients. In an out-of-hospital randomized controlled trial by Schreiber et al., [27] hypotensive resuscitation was shown to be feasible and safe in 192 blunt and penetrating trauma patients. A non-significant difference in mortality was reported in the prospective, 2-arm, randomized controlled trial by Carrick et al. [28] comparing a MAP target of >50 mmHg to a MAP >65 mmHg for patients with penetrating trauma who presented with hypotension (SBP <90 mmHg). Recent systematic reviews on this topic have concluded that mortality for trauma patients appears to be improved when permissive hypotension is employed [29]. While the optimal blood pressure target has yet to be defined, based on the currently available data, a SBP of 90 to 100 mmHg is likely safe for most patients [30]. For patients with traumatic brain injury or spinal cord injuries, higher blood pressures are recommended and hypotensive resuscitation should not be used in these patients. According to the latest guidelines for the management of traumatic brain injury, a SBP >100 mmHg is recommended for patients aged 50 to 69 and a SBP >110 mmHg is recommended for patients younger than 49 or older than 70 years [31].
AIRWAY MANAGEMENT
Airway management is a critical component to the resuscitation of critically ill trauma patients and a key component of DCR. Patients that arrive at the hospital with major trauma and severe metabolic derangements require definitive airway control. The timing of airway management is critical, and must balance the advantage of resuscitation before induction to minimize the risk of post intubation cardiac collapse vs the need for rapidly controlling the patient’s physiology, including the respiratory system.
Rapid sequence intubation is the standard technique for intubation in most trauma patients. Medications and doses need to be carefully considered and individualized for hypotensive trauma patients. Care must be taken to balance the need for sedation and pain control vs the hemodynamic effects of the medications. Medication options include sedatives and analgesics as well as a paralytic. While a full discussion of different medications and doses is outside of the scope of this article, a brief discussion of common medications is depicted in Table 1 [32]. In the hypotensive patient, lower doses of sedation are usually given while higher than normal doses of paralytics can be used to decrease the time to onset [33]. It is important, when possible, to briefly resuscitate patients before administrating any agent.
When controlling an airway, any patient with significant blunt trauma is presumed to have a cervical spine injury. Using difficult airway algorithms [34,35] for some patients with blunt and penetrating trauma to the head and neck may help. There should be a low threshold for early surgical cricotomy.
SURGICAL DAMAGE CONTROL
Damage control surgery minimizes the amount of time and initial procedures done in the operating room to only critical interventions. This includes controlling major hemorrhage, containing contamination, and applying temporary closure devices. Techniques such as abdominal packing, the use of hemostatic agents, vascular shunting, and use of endovascular stenting and embolization may help. The goal is to minimize time in the operating room, limiting further bleeding and heat loss to allow time for the patient to be resuscitated in an intensive care unit to correct physiological and metabolic derangements before a planned return to the operating room. The return to the operating room can be planned for between 6 and 48 hours. Changing patient conditions may require earlier re-exploration. The return operating room visit will be for definitive repair and closure [36-39].
INTRAVENOUS FLUID VERSUS BLOOD
The practice of crystalloid fluid resuscitation was supported by 1960’s data which suggested a hemorrhage was associated with a loss of isotonic fluid in the extracellular space [40]. This fluid deficit could be readily replaced with isotonic crystalloid. However, there is a growing body of literature highlighting the harms of crystalloid fluids in shock states, and, specifically, in major trauma [41]. Crystalloid fluid promotes acidosis, dilutes coagulation factors, and disturbs inflammatory mediators.
The harms of crystalloid resuscitation in trauma patients are well documented. A retrospective study by Ley et al. [42] demonstrated that emergency department administration of greater than 1.5 L of crystalloid in trauma patients was associated with increased mortality. In another retrospective study, Neal et al. [43] demonstrated that a crystalloid (liter):packed red blood cell (unit) ratio of greater than 1.5:1 in patients who had received massive transfusion was associated with a 70% higher risk of multiple organ failure, and a two times greater risk of acute respiratory distress syndrome and abdominal compartment syndrome. More recently, the administration of prehospital plasma was studied in a large prospective multicenter cluster randomized trial which compared prehospital resuscitation with thawed plasma vs standard care. It demonstrated a significantly lower mortality at 30 days than the standard care group (23% vs. 33%, P=0.03) [44].
TRANSFUSION RATIOS
Contributions to the military and civilian trauma literature in the early 2000’s suggested a benefit to increased plasma:pRBC and platelet:pRBC ratios in massive transfusion protocols. However, the optimal ratio of blood components was not yet clearly defined [7,45-53]. In 2013, the PROMMTT study group performed a prospective cohort study demonstrating that higher plasma:pRBC and platelet:pRBC ratios conferred survival benefits in the first 6 hours. Patients with ratios below 1:2 were 3 to 4 times more likely to die than patients with ratios greater than 1:1 [54]. In 2015, the PROPPR study group performed a large, multicenter, randomized control trial comparing ratios of plasma, platelets, and pRBC’s in a 1:1:1 versus 1:1:2 ratio. While there were no significant differences in mortality at 24 hours or 30 days, more patients in the 1:1:1 group achieved hemostasis, and fewer died of exsanguination in the first 24 hours [55].
Cryoprecipitate is a pooled human blood product which contains fibrinogen, factor VIII, factor XIII, vWF, and fibronectin. It is included in many current massive transfusion protocols. Most patients in the PROMMTT trial did not receive cryoprecipitate, but, in those who did, there was no in-hospital mortality benefit [56]. However, in a retrospective review of the MATTERs II Study cryoprecipitate was found to independently add to the survival benefit of transexamic acid in major trauma [57]. There also may be a role for using thromboelastography (TEG) or rotational thromboelastometry (ROTEM) to guide cryoprecipitate administration in trauma, but more study is needed to make specific recommendations [58].
WHOLE BLOOD
Fresh whole blood (FWB) is an attractive transfusion product as it contains all components required for coagulation. Moreover, the logistics of massive transfusion are streamlined as, in a hemorrhaging patient, FWB simply replaces lost blood in a single transfusion product.
FWB resuscitation was born out of necessity in military conflicts. During the early years of the wars in Iraq and Afghanistan, FWB was used during massive transfusion at combat support hospitals when blood components (especially perishable platelets) were scarce [59]. The military maintains a “walking blood bank” of service members. FWB is a readily available balanced transfusion product for resuscitation of combat victims. Between 2003 and 2007 over 6,000 units for FWB were transfused in Afghanistan and Iraq, approximately 4% of blood products transfused during this time period [60]. Retrospective analysis of this experience demonstrated potential survival benefit of FWB in resuscitation. Spinella et al. [61] performed a retrospective analysis of 354 combat casualty patients and compared those who received FWB, RBC’s, and plasma but not platelets vs those who received RBC’s, plasma and platelets but not FWB. Both 24-hour survival (96% vs. 88%, P=0.018) and 30-day survival (95% vs. 82%, P=0.002) were improved in the group who received FWB. The mortality benefit of FWB may be from the potential deleterious effect of anticoagulant additives in stored component therapy.
The safety of FWB in both military and civilian settings is well documented. The risks of infectious disease transmission related to FWB transmission can be effectively mitigated with rapid pretransfusion screening tests [62]. Cold stored whole blood was evaluated by Yazer et al. [63] for use in a civilian academic level 1 trauma center; 47 patients were transfused a mean of 1.74 units of whole blood (mean age of the units was 7.74 days) without any adverse reactions. There is a risk of administering donor leukocytes in transfusion recipients known as transfusion associated microchimerism associated with blood transfusion in trauma. This risk is postulated to be greater with transfusion of FWB, but has not been confirmed [64,65].
While the use of FWB in trauma is promising, at the present time, the role of FWB is primarily as a transfusion product when complete component therapy is unavailable. While apheresis platelets have become readily available at major combat hospitals, a study by Perkins et al. showed no survival difference between combat victims receiving apheresis platelets versus FWB [66]. FWB may additionally have a role in transfusion to address the coagulopathy of major trauma [67].
TRANEXAMIC ACID
In normal fibrinolysis, plasminogen binds to lysine on the surface of fibrin. Tissue plasminogen activator then converts plasminogen to its active enzymatic form, plasmin. Plasmin degrades fibrin to inactive fragments, and degrades the formed clot. Tranexamic Acid (TXA) is synthetically derived from the amino acid lysine. TXA blocks the lysine binding sites on the surface of plasminogen and, in doing so, reversibly inhibits the fibrinolytic interaction between plasminogen, plasmin, and fibrin [68].
Both intravenous and oral TXA have a well-documented history of safety and efficacy in preventing blood loss. Accepted applications include cardiac surgery, upper gastrointestinal hemorrhage, traumatic hyphema, oral surgery, gynecologic surgery, and blood loss from menorrhagia [69-77].
With a large body of evidence to support the use of antifibrinolytic therapy for the prevention of blood loss from disordered coagulation, there was significant interest in the role TXA may have in trauma. In 2010, the CRASH-2 trial, a large, randomized controlled trial across 40 countries with 20,211 enrolled patients studied the administration of 1 g of TXA over 10 minutes followed by an infusion of 1 g over 8 hours within 8 hours of injury in adult trauma patients with, or who were at risk of, significant bleeding. Using an intention to treat analysis, TXA administration was associated with a reduction in all-cause mortality (14.5% vs. 16.0%, P<0.001), and a reduction in the risk of death due to bleeding (4.9% vs. 5.7%, P<0.001) [78].
The findings from the CRASH-2 trial were supported by the MATTERs study—a retrospective observational study of soldiers resuscitated after combat injury in a surgical hospital in southern Afghanistan which compared TXA administration against control. There was a reduction in unadjusted mortality in the TXA group over the no TXA group (17.4% vs. 23.3%, P=0.03). The benefit from TXA was the greatest in patients who received massive transfusion (14.4% vs. 28.1%, p<0.001) [79].
The exact mechanism by which TXA confers a survival benefit in trauma is unclear. The CRASH-2 trial demonstrated no significant difference in the rate of RBC transfusion between the two groups [80]. Moreover, a subsequent exploratory analysis of the data from the CRASH-2 trial found that the survival benefit from TXA in trauma was only in patients who received TXA within 3 hours from the time of injury, and an increase in the risk of mortality due to bleeding in those who received TXA greater than 3 hours from time of injury [81]. In patients undergoing cardiac surgery, TXA has been shown to attenuate the host inflammatory response, which has been offered as an alternate mechanism to explain the benefits of TXA in trauma [82-84].
THROMBOELASTOGRAPHY
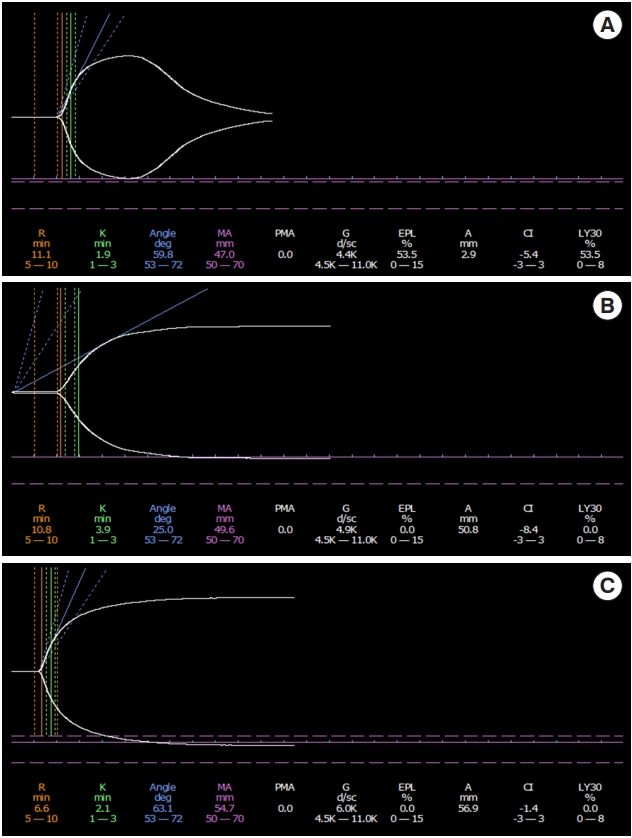
TEG is a technique used for the characterization and quantification of status of a patient’s coagulation state. The technique involves placing a small amount of the patients blood in a cuvette which rotates at a fixed rate with a pin that is placed into the sample. Two major platforms the TEG and the ROTEM are currently in use. They differ mainly in if the sample or the pin rotate. Additional reagents can be added to speed up the process or overcome heparin. The TEG can be used to measure hemostasis by studying the strength and elasticity of the clot and how quickly the clot breaks up. Main measurements, normal values and treatments are summarized in Table 2 [85]. TEG can be viewed in realtime and management decisions about blood products can be tailored to the patient. Normal, hypercoagulable, hypocoagulable, and hyperfibrinolytic tracing can be seen in Figure 4.
RESUSCITATIVE ENDOVASCULAR BALLOON OCCLUSION OF THE AORTA
Resuscitative endovascular balloon occlusion of the aorta (REBOA) is a minimally invasive aortic cross clamp that can be used to control none compressible torso and pelvic bleeding. Newer generation devices use a 7-fr arterial sheath for cannulation of the common femoral artery. This can be done either percutaneously or by femoral cut down. Depending on the site of injury the balloon can be inflated in either Zone 1 at the level of the diaphragm for intrabdominal hemorrhage or Zone 3 at the bifurcation of the aorta for pelvic hemorrhage. A recent Joint statement from the American College of Surgeons Committee on Trauma and the American College of Emergency Physicians on the clinical use of REBOA has started to establish an approach to implementation of a REOBA program [86]. The basic endovascular skills for trauma course has been used to teach the placement and use of the REBOA catheter. Additionally, the Aortic Occlusion for Resuscitation in Trauma and Acute Care Surgery registry is a prospective effort to collect data on the use and outcomes of REBOA to better understand how and when the REBOA should be used.
CONCLUSION
Damage control is a term coined by the Navy. Its principles have been adapted by the trauma community for use in the most severely injured patients. Damage control is more than a single technique or treatment but rather many strategies that combine resuscitation and surgical care. It focuses on rapid resuscitation with blood, rapid hemorrhage control, and correction of metabolic derangements. When correctly utilized it has been shown to improve survival, decrease length of stay, and improve outcomes.