INTRODUCTION
There is a high occurrence of burnout among healthcare providers, including nurses, physicians, pharmacists, residents, and even medical students [1-4]. High burnout among healthcare providers is associated with significant negative outcomes, including decreased job satisfaction, professional dropout, increased medical errors, increased risk of suicide, and substance abuse [5-8]. Emergency medicine (EM) providers typically work in a more stressful environment and risk higher rates of litigation as compared to other healthcare specialists. As a result, they tend to suffer a higher burnout rate and incidences of burnout related outcomes [6,9,10].
Many interventions focusing on provider wellness have been reported in the literature to help prevent and ameliorate provider burnout [11-13]. Increasing general self-efficacy, reducing financial debt, receiving more perceived social support, and developing a better culture of wellness are some interventions that have proven to reduce provider burnout [2,14,15]. However, these claims appear to be more specialty specific, with very few applicable to EM due to limited sample size, thereby lacking generalizability and large-scale external validations.
Wellness culture can be characterized by several domains. It consists of provider value alignment, perceived appreciation, leadership quality, and provider social support. Studies focused on wellness culture found that a positive culture increases provider performance, increases job security and satisfaction, and reduces provider burnout [16,17]. Each individual wellness culture domain has been reported previously in the literature. However, the findings are not consistent, and each study seemed to focus on different domains. A study done by Jambrak et al. [18] in Australia reported that aligning personal values with organizational values can improve job satisfaction, lower the intention to leave, and reduce burnout. However, another study done by Healthy Work Place Investigators in the US found that although clinicians with a high degree of trust are associated with high value alignment, no significant difference occurred in terms of its association with clinician burnout [19]. Shanafelt et al. [20] and Shanafelt and Noseworthy [21] considered that the cause of burnout is not solely based upon the individual physician, rather it is a systemic issue. Therefore, executive leadership plays an important role in promoting engagement and reducing burnout. Wu et al. [17] also reported that provider work-family conflicts positively affect job burnout. On the other hand, these studies focused on general practitioners and internal medicine specialists at academic centers. Therefore, it is still uncertain whether such findings can be replicated in EM with different types of EM providers practicing in different healthcare settings (i.e., academic versus community, high versus low volume emergency department [ED), etc.). In addition, most studies focused on one or two wellness culture domains, rarely considering different domains as an integrated entity. Few provided insight as to the potential interactions among different domains. We believe it is also necessary to determine whether each domain acts as an independent factor that protects against provider burnout.
A better understanding of provider wellness culture could help foster a provider wellness strategy that optimally suits provider needs, with interventions that more effectively reduce provider burnout. Reduced burnout levels would also lead to better patient-centered care. Therefore, due to the lack of sufficient data describing EM provider wellness culture in relation to burnout, we aim to conduct a multi-center observational study to determine the association between ED provider burnout and different wellness culture domains, and delineate the optimal domains from wellness culture that protect against EM provider burnout.
METHODS
Study design and setting
This was a secondary data analysis of a previous quality improvement project focusing on healthcare provider wellness. Data were collected prospectively via a Stanford Wellness online survey from January to March 2018. The survey questionnaires were provided by the Stanford WellMD Center using Qualtrics Survey software (Provo, UT, USA). We had a contractual agreement with permission to use data for secondary analysis. The survey was sent to all ED physicians and advanced practice providers (APPs). Healthcare providers were from sixteen different hospital EDs located regionally within North Texas, USA. Among the sixteen EDs, two have extremely high annual volumes (>100,000 visits/yr), in which one is an academic urban ED with an Accreditation Council for Graduate Medical Education accredited EM residency program and the other is a community urban ED. Five EDs have moderate to high annual volumes (60,000ŌĆō100,000 visits/yr), while the other nine EDs have low to moderate annual volumes (30,000ŌĆō60,000 visits/yr). Due to the nature of secondary data analysis with deidentified personal information, this study was waived for approval by the local institutional review board. Due to the nature of secondary data analysis, this study was waived for approval from local institutional review board.
Study participants
We included surveys from all qualified ED healthcare providers from sixteen different EDs who agreed to participate in this study. We excluded surveys from providers who declined to participate, empty surveys, incomplete surveys (<10% complete), and duplicate surveys.
Wellness culture measurements
In this study, wellness culture was classified and measured across the six categories listed below based on several previous studies [7,22-24]. First, organization or personal value alignment to demonstrate the understanding of organizational value, sense of belonging or teamwork, as well as the value of personal work. Second, perceived provider appreciation to assess whether a healthcare providerŌĆÖs work was appreciated by their team members, supervisors, and their family. Third, leadership quality to measure overall satisfaction with a providerŌĆÖs supervisor in different areas (e.g., career development, empowerment, encouragement, respect, providing helpful feedback, etc.). Fourth, healthcare providers control over schedule to determine whether an individual provider is able to control their own work schedule. Fifth, peer support to measure a variety of support resources from team members (e.g., peer listening/empathy, providing solutions, lifting providers up, helping with providerŌĆÖs work, etc.). Sixth, family support to recognize special needs, including pregnancy needs, breast feeding/pumping needs, parental leave, and leave to care for a family member.
All of these items were graded on a 5-point Likert scale ranging from 0 (not at all, strongly disagree/dissatisfied) to 4 (completely, strongly agree/satisfied). Some items could be answered as not applicable (e.g., special needs). The overall score of each category was calculated by averaging the total item scores. If items were answered as not applicable, such items were excluded from the calculation. High scores indicated provider strong agreement or satisfaction with a given culture of wellness, whereas low scores indicated the opposite.
Outcome measurements
Healthcare provider burnout was measured as the study outcome. We used a 10-item questionnaire to measure healthcare provider burnout (Appendix 1). This burnout tool was adapted partly from a 16-point Professional Fulfillment Index covering two distinct domains (emotional exhaustion and interpersonal disengagement) [7]. It is also similar to the Maslach Burnout Inventory, a common burnout assessment tool used in the literature [25]. Each item was scored on a 5-point Likert scale ranging from 0 (not at all/strongly disagree) to 4 (extremely/strongly agree). The overall burnout score was calculated by averaging the total item scores.
Variables
Provider demographics included age, sex (male or female), race (White, Black or African American, Asian, or other), and ethnicity (Hispanic/Latino or not Hispanic/Latino). Providers listed their primary practice ED. EDs were divided into three volume groups (high, >100,000 visits/yr; moderate, 60,000ŌĆō100,000 visits/yr; low, 30,000ŌĆō60,000 visits/yr). In general, there was less than 2% missing data among all variables except the ŌĆ£family supportŌĆØ domain. Since this domain mainly surveyed provider needs under special circumstances (e.g., pregnancy, breast feeding, parental leave, etc.), the number of ŌĆ£not applicableŌĆØ answers were significantly large (Appendix 2). Therefore, multiple imputation was applied to handle these missing data.
Data analysis
Analysis of variance was used for continuous data comparisons among groups, whereas Wilcoxon rank sum test was used for categorical comparisons. We used skewness and kurtosis to determine whether each wellness culture domain score was normally distributed. |Skewness| <0.5 was mildly to normally distributed, 1> |Skewness| Ōēź0.5 was moderately skewed, and |Skewness| Ōēź1 was highly skewed. Kurtosis >3 was considered data less normally distributed. We used CronbachŌĆÖs alpha (╬▒) to determine internal consistency of each wellness culture domain measurement. An ╬▒>0.8 was considered good reliability and ╬▒>0.7 was considered adequate reliability. To determine the association between burnout and culture of wellness, we initially used correlation co-efficiency (r) with |r| Ōēź0.5 indicating strong correlation, 0.5> |r| Ōēź0.3 indicating moderate correlation, and 0.3> |r| Ōēź0.1 indicating weak correlation. Meanwhile, we initiated a univariate logistic regression to determine the association between burnout and each domain of wellness culture. Then, we fit a multivariable logistic regression model evaluating such associations with different domains of wellness culture, different roles of ED providers (physician versus APP) and different ED settings (high versus moderate versus low volume EDs) after adjustment for provider sex, age, race, and ethnicity. We determined providers of high burnout with burnout scores of more than 1 based on our providers consensus by using a modified Delphi technique along with previous similar reports [26-28]. Risk predictors of burnout were determined with adjusted odds ratios with 95% confidence intervals (CIs). All analyses were performed using Stata ver. 14.2 (StataCorp., College Station, TX, USA) with P-value <0.05 considered statistically significant.
RESULTS
A total of 242 surveys collected from January to March 2018 were placed in the final analysis. Table 1 shows the general characteristics of the study participants. Our study included 146 ED physicians and 96 APPs. Most physicians were males while most APPs were females. Most participants were White, non-Hispanic, and practicing at moderate to high volume EDs. More than half of the providers (56% from physicians and 50% from APPs) showed high burnout levels. However, no significant differences in terms of burnout levels between physicians and APPs were found (Table 1).
The six different wellness culture domains included organizational/personal value alignment (referred to as value), perceived appreciation at practice site (referred to as appreciation), leadership/experience with the supervisor (referred to as leadership), control over schedule (referred to as schedule), peer support (referred to as peer), and family support (referred to as family). Provider burnout scores and scores of their wellness culture domains are reported in Table 2. Data from wellness culture domains and burnout assessment were mildly skewed. Therefore, both mean score with standard deviation and median score with interquartile range were reported. Internal consistency was measured among different wellness culture domains using CronbachŌĆÖs ╬▒; all showed good internal consistency (Table 2).
To determine whether burnout was associated with different ED providers and ED settings, ED providers were divided into physicians and APPs and ED settings were divided into high, moderate, and low volume groups based on annual ED volumes. No statistical significance occurred in terms of ED provider burnout levels when different ED providers and ED settings were compared (P>0.05) (Table 3).
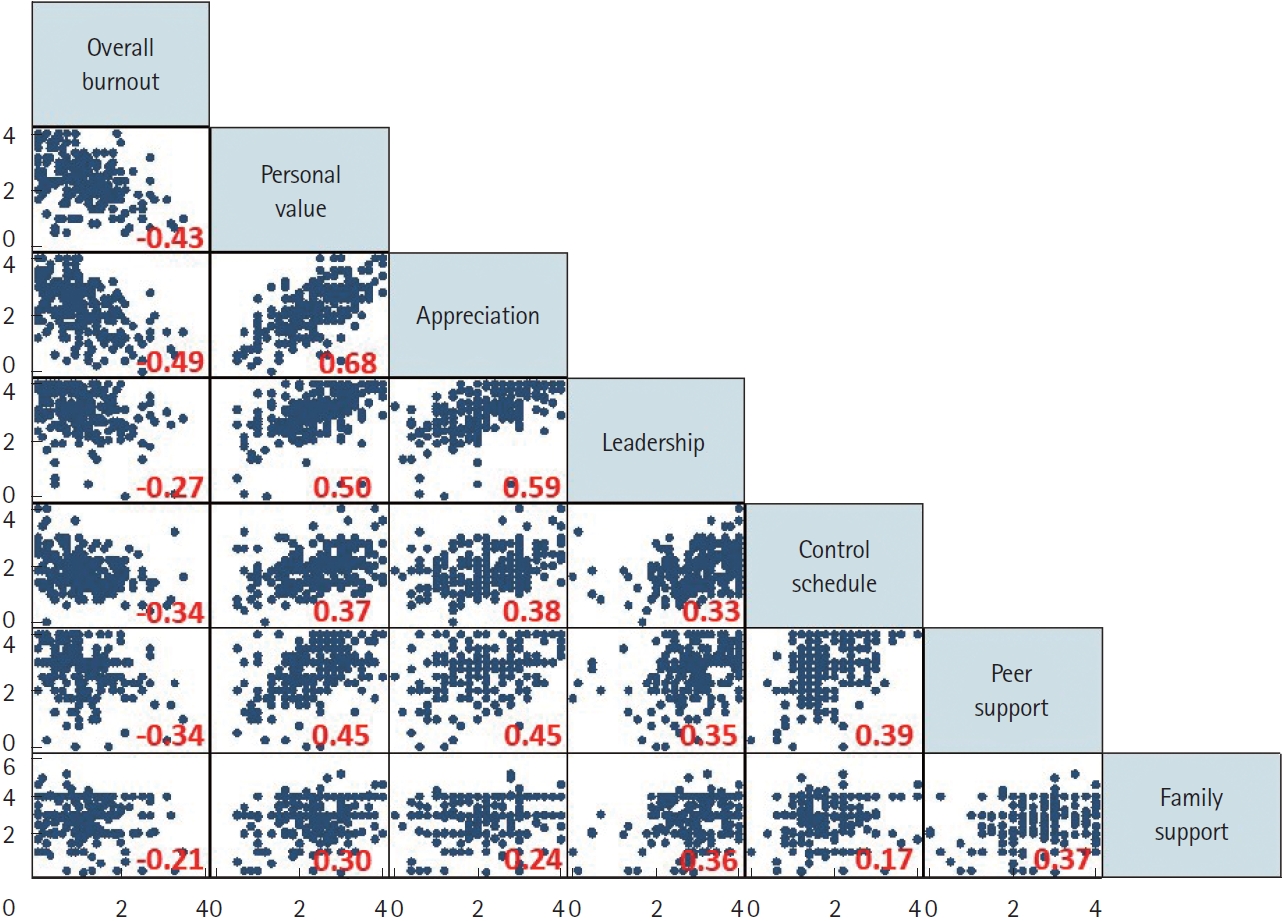
Fig. 1 shows correlations between burnout and different wellness culture domains. Moderate correlations (>0.3) were found between burnout and four of the provider wellness culture domains (value, appreciation, schedule, and peer). High correlations (Ōēź0.5) were found among three wellness culture domains (value, appreciation, and leadership). Weak correlation was found between burnout and family support (Fig. 1).
To further determine the associations between burnout and provider wellness culture, both an unadjusted univariate logistic regression and adjusted multivariate logistic regression analysis were performed. All wellness culture domains showed certain associations with provider burnout by univariate regression analysis. However, when analyzed using multivariate logistic regression, only appreciation and family support domains were found to protect provider burnout significantly (Table 4). In addition, different ED providers and different ED settings seemed to have no direct association with provider burnout after all confounders were adjusted (e.g., age, sex, race, ethnicity) (Table 4).
DISCUSSION
Healthcare provider burnout has been studied frequently in recent years and is related to the quality of patient care delivered [29]. Different interventions implemented to help ameliorate healthcare provider burnout have also been reported with diverse outcomes [18,19]. However, EM provider wellness culture has not been widely studied and little is known of the impact of wellness culture on EM provider burnout. In order to determine the optimal intervention for EM provider burnout prevention and potential amelioration, we investigated the role of EM provider wellness culture in relation to burnout. In this study, we found that ED providers had comparable burnout levels to those of healthcare providers in prior studies [10,30]. Some cultures of wellness areas showed moderate correlation with provider burnout. These areas included organizational/personal value alignment, provider appreciation, control over schedule, and peer support. However, when analyzed together, only provider appreciation and family support were found to have protective effects on EM provider burnout. Our study systematically analyzed how different wellness culture domains impacted provider burnout, identified its correlations, and determined the independent domains potentially affecting provider burnout. Such analyses have not been extensively reported in the current literature. Effectively screening for burnout and providing useful interventions for burnout prevention are very important steps in physician wellness, especially in the field of EM, a specialty with a high burnout rate. Setting up work-life balance, receiving peer and leadership support, and recognizing appreciations, which are part of the ŌĆ£wellness cultureŌĆØ, have been reported separately to ameliorate burnout to certain levels from different studies [21,31]. Our study provides comprehensive analyses using all the wellness culture domains to determine their association and interactions with provider burnout. Our study findings add evidence to the literature pool relative to optimizing potential effective interventions from wellness culture to help ameliorate ED provider burnout. More specifically, such findings seem to be general regardless of the different roles of EM providers (physician versus APP) or ED settings (high versus moderate versus low volumes).
Our findings indicate that ED healthcare providers have a high burnout rate, which is consistent with other studies [10,30]. Different burnout rates obtained from different burnout assessment tools could be due to different thresholds set in different studies [7,28]. Our study also shows moderate correlations between burnout and most wellness culture domains. Provider appreciation is one of the wellness culture domains that significantly affect healthcare provider burnout. This has been cited in a previous report [32], yet it has not been systematically studied. Appreciation seems to bring EM providers more happiness, better job satisfaction, and results in high staff retention [33,34]. This factor might effectively reduce provider anxiety and emphasize provider value at work, thus indirectly ameliorate their burnout. Family support seems to be another provider wellness culture domain that could potentially protect against provider burnout. Work-family balance has been emphasized and proven to be associated with burnout [17,35]. Social support including family support has been investigated and validated to interfere with provider burnout [36,37]. Female physicians burdened with high risk pregnancies and miscarriages tend to experience higher burnout rates [36]. Whereas, resources at the institutional level including providing adequate breast pumping time is considered a successful strategy to support physician mothers in their careers [37]. Our study extended such findings in EM. Other areas of wellness culture, though highly correlated with burnout (value, appreciation, and leadership), did not prove to independently affect provider burnout when analyzed together. This might be due to higher correlations among these factors (rŌēź0.5, appreciation versus value versus leadership (Fig. 1). Others, such as control over schedule, or peer support, which could play important roles in minimizing provider burnout, although statistically not significant, could have synergetic effects on provider appreciation (Appendix 3). However, due to a lack of strong data to support this hypothesis we are unable to explain its mechanisms thoroughly in this study. More specific studies focusing on the interactions among all these wellness culture areas are warranted in the future.
In this study, we also found provider burnout was not significantly impacted by providers working at different ED settings. In general, providers with longer-hours worked or overloaded work might suffer more stress, which could potentially result in higher burnout [38,39] However, it is still unknown as to whether EM providers working in different ED settings have different levels of burnout. Our study showed no differences when comparing providers working at different ED settings. In addition, no burnout difference was found among physicians in comparison to APPs. This might be explained due to the different definitions of ED settings. In this study, we defined annual patient visits of less than 60,000 as low volume, which is different than that defined in the Emergency Department Benchmarking Alliance report [40]. This studyŌĆÖs definition is based on the fact that we have no ED within this system with an annual volume of less than 30,000 visits. Even when reclassifying all EDs into two categories (high versus moderate), our findings are still consistent with the current report (Appendix 4). Another possible reason might be due to individual provider workload although providers working at relatively low volume EDs carried similar workloads (patients per hour) when compared to providers working at relatively high volume EDs (data not shown). Therefore, we believe working at different ED settings might not be an independent critical issue affecting provider burnout.
Our study has its limitations. Since this is a retrospective observational study with secondary data analysis, patient selection bias, missing data, and inaccurate information may inevitably exist. Although this study enrolled providers from sixteen different EDs across North Texas, our sample size is small, and our findings might still be less generalizable. Additionally, provider culture of wellness could include a multitude of other domains not investigated in this study; simply analyzing six different domains might not be enough. Finally, provider burnout could be affected multi-factorially, and due to limited data, we are unable to analyze all the confounders which may skew our results. Therefore, in order to accurately determine the association between EM provider burnout and culture of wellness, a large-scale multi-center prospective study is warranted for further validation.
In conclusion, ED providers have a relatively high burnout rate. Provider burnout might have certain associations with wellness culture. Provider appreciation and family support seem to play important roles in provider burnout protection.