INTRODUCTION
Patients with maxillofacial trauma occasionally present serious challenges for physicians due to several factors. Two major factors that should be considered by a physician are airway maintenance and bleeding control [1,2]. Airway maintenance is easily compromised by fracture of the surrounding bony tissue and/or swelling of soft tissues [1]. In particular, any injury associated with the soft palate is difficult to compress and control bleeding due to its anatomical characteristics.
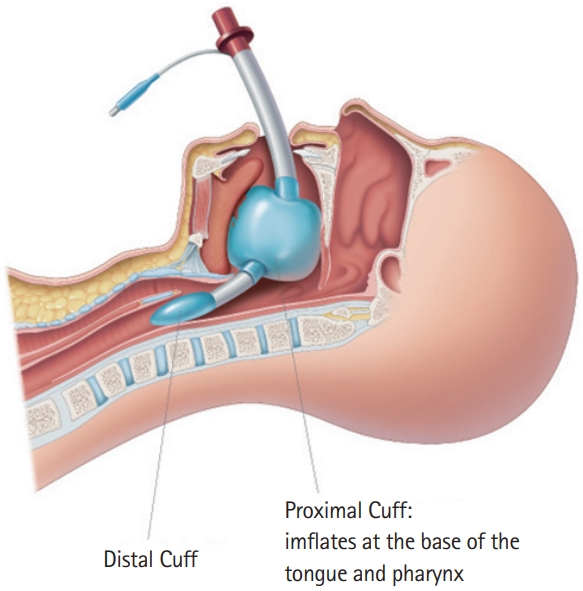
We used an alternative airway device consisting of a pharyngeal balloon, King laryngeal tube (LT) (King Systems Corp., Noblesville, IN, USA) to control the intractable bleeding and prevent airway obstruction due to a hematoma associated with orofacial trauma. The King LT is a supraglottic airway device composed of a simple airway tube with an oropharyngeal and esophageal balloon [3]. Its location of sealing is the base of the tongue, and the sealing mechanism is an inflatable balloon. In addition, it can protect the airway from aspiration with the said esophageal balloon. In our attempts, King LT was effective in controlling bleeding and preventing airway obstruction. In this article, we report two cases treated using this device. The patients provided informed consent for publication of the research details and clinical images.
CASE REPORT
Case 1. Blunt trauma case
The patient was a 53-year-old male with a history of hypertension, diabetes mellitus, and end-stage renal disease. He was brought to the emergency department after being hit by a car while riding his bicycle.
On physical examination, the patient was alert, and his general appearance was good. Upon arrival at the emergency department, the patient’s blood pressure was 170/90 mmHg, pulse rate was 90 beats per minute (bpm), respiratory rate was 14 breaths/min, and body temperature was 36.0°C. The patient complained of facial pain and intraoral bleeding, and a hematoma and pulsatile bleeding were observed on his soft palate (Fig. 1). Anemia was present in the patient’s initial laboratory findings, with a hemoglobin concentration of 6.6 g/dL and a hematocrit value of 18.8%. Approximately 1 hour later, the patient became drowsy, and his hemodynamic status became unstable. At this point, his blood pressure was 87/61 mmHg, and his heart rate was 104 bpm. Endotracheal intubation and blood transfusion were performed; however, the patient’s hemodynamic status remained unstable. His soft palate was examined, and active pulsatile bleeding was noted. Sengstaken-Blakemore (S-B) tube insertion into the oral cavity was attempted at first, but it failed to control the bleeding. Of the two tube pieces constituting the S-B tube, the esophageal balloon was not used, and the gastric balloon was placed in the oropharyngeal cavity and then inflated by about 100 mL. We removed the S-B tube and inserted a King LT of size 4, which is an average adult size, and 60 to 80 mL of air, which is normally injected in conjunction with a size 4 device, was injected into the oropharyngeal balloon (Fig. 2). Subsequently, the active bleeding of the soft palate was stopped, and the patient became hemodynamically stable. His blood pressure increased to 130/60 mmHg, and his pulse rate dropped to 95 bpm after 30 minutes. Computed tomography imaging of the neck showed a right soft palate laceration and swelling of the adjacent structures (Fig. 3).
The King LT was removed the next day. On day 6 after admission, the patient was taken off the ventilator, and his soft palate laceration was sealed off spontaneously. The patient was discharged from the hospital on day 21 without any complications.
Case 2. Knife injury case
The patient was a 36-year-old male who had been stabbed in zone 3 of the neck. Upon arrival at the emergency department, his vital signs were stable. The patient presented with a drowsy mental status and intraoral bleeding. The inlet size of the stab wound was 3 cm, while the depth of the stab wound was not exactly measured; however, his sustained oral bleeding warranted the rough assumption of a through-and-through stab wound of the neck.
Computed tomography imaging (Fig. 4) revealed airway narrowing due to a hematoma and soft tissue swelling, and total airway obstruction was deemed imminent. There were four failed endotracheal intubation attempts due to his narrowed airway and sustained oral bleeding. Therefore, the King LT of size 4 was used as an emergency countermeasure, and 60 to 80 mL of air was injected into the oropharyngeal balloon. After securing airway maintenance via insertion of the King LT, the otolaryngologist who performed the operation voiced concerns that airway maintenance would fail while manipulating the King LT during the operation, so we discussed measures together. Ultimately, cricothyroidotomy was performed on the patient to protect airway maintenance during the operation (Fig. 5). With this status, the patient was brought to the operating room.
In the operating room, the stab wound on the neck was explored. A bleeding site in the left lateral oropharynx was identified, but the opening site was not found. As a result, the bleeding site in the oropharynx was packed with TachoComb (CSL Behring, Tokyo, Japan), and a Penrose drain was placed to allow drainage of the wound.
On day 6 after admission, the patient was taken off the ventilator. He was discharged from the hospital on day 29.
DISCUSSION
An orofacial injury can be life-threatening. This is a rare occurrence involving both irreversible shock and airway obstruction in some cases [2]. In such a case, it is difficult to control the bleeding and prevent airway obstruction by conventional treatment. The patient can also become hemodynamically unstable [1,4]. Transcatheter arterial embolization and other operative techniques are considered effective methods for controlling arterial bleeding [5]; however, they focus solely on managing arterial bleeding, not venous bleeding. Further, such methods are not always carried out immediately in all institutions due to the limited time allowed for preparation [4-8].
The King LT was used in both of our cases. It was developed as an alternative airway device for patients with difficult airways; however, its structural characteristics offer an additional function. In both cases, the device’s inflated balloon took on the role of a compressor, and the King LT acted as an airway-maintenance device (Fig. 6). In our hospital, the King LT was used as it was available. For adults 155 to 180 cm in height, size 4 of this device is typically used, and the oropharyngeal balloon in the King LT is inflated by 60 to 80 mL with 60 mmH20. Similar to the King LT, a supraglottic airway device with a ballooning structure in the oropharynx can be placed as an alternative. Conversely, supraglottic airway devices that do not have a ballooning structure in the oropharynx cannot be used for the purpose outlined in our cases.
As previously mentioned, the described hemostatic method incorporating the King LT is a simple treatment that can be available in underequipped institutions. There are many balloon catheters that can act as compressors (e.g., an S-B tube or a Foley catheter) [8]. Among them, the S-B tube is more advantageous for controlling nasal cavity bleeding due to the long cylindrical structure of its balloon, but it is unfavorable for controlling oropharyngeal cavity bleeding. In addition, compared to the King LT, the S-B tube has the disadvantage of requiring additional procedures to protect the airway. The Foley catheter has a balloon size of 10 or 30 mL, which is too small for the adult oropharyngeal cavity. There have been attempts to use alternative airway devices, such as the laryngeal mask airway (Intavent Orthofix, Maidenhead, UK) and various surgical airway-management methods (e.g., submental intubation, cricothyroidotomy) [1,9]. Although such devices can ensure airway maintenance, they are not suitable for oropharyngeal bleeding control because they do not have a structure that can inflate while applying adequate pressure to the oropharynx.
However, supraglottic airway devices with a balloon structure in the oropharynx, like King LT, can function as a compressor simultaneously with an airway device. Intubation of patients with orofacial injuries is difficult because such injuries obstruct the visual field, increasing the difficulty of inserting two tubes, i.e., for preventing airway obstruction and bleeding control, respectively [1]. Under these circumstances, the King LT device can be considered a useful management tool for patients with massive orofacial bleeding and hematomas that are uncontrollable via conventional treatment [6,8].
In conclusion, our cases contribute evidence to the literature that a LT with an inflatable balloon, including the King LT, can be effective in managing life-threatening orofacial injuries. Furthermore, such a device is applicable in institutions where surgical treatment is not possible due to inadequate equipment. Prospective randomized studies are needed to further assess the effectiveness of a LT with an inflatable balloon in life-threatening orofacial injuries.